Camilo Ramírez-Giraldo, Sofía Santamaría-Forero, Isabella Van-Londoño, Jorge Navarro-Alean, Carlos Figueroa-Avendaño, Susana Rojas-López, Laura Carolina Camacho, Andrés Isaza-Restrepo
{"title":"Type of mesh and wall plane in prophylactic mesh after stoma closure: A network meta-analysis.","authors":"Camilo Ramírez-Giraldo, Sofía Santamaría-Forero, Isabella Van-Londoño, Jorge Navarro-Alean, Carlos Figueroa-Avendaño, Susana Rojas-López, Laura Carolina Camacho, Andrés Isaza-Restrepo","doi":"10.1007/s10029-025-03413-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Prophylactic mesh placement lowers incisional hernia risk, but the ideal mesh type and anatomical plane remain unclear. This study aims to determine which mesh and placement site are associated with the lowest rates of incisional hernia and surgical site infection after stoma closure.</p><p><strong>Methods: </strong>A systematic review of PubMed, the Cochrane Library, and Embase was conducted to identify comparative studies evaluating the type of mesh and/or the anatomical plane of mesh placement in the abdominal wall following stoma closure for the prevention of incisional hernias. A network meta-analysis was performed to assess incisional hernia and surgical site infection.</p><p><strong>Results: </strong>We included 11 included studies involving 2,148 patients. The use of prosthetic mesh (OR = 0.137, 95%CI 0.056-0.335), bioprosthetic mesh (OR = 0.171, 95%CI 0.061-0.473), and biological mesh (OR = 0.528, 95%CI 0.336-0.828) was associated with a lower risk of incisional hernia compared to no mesh use. Mesh placement in a retromuscular position (OR = 0.068, 95%CI 0.024-0.189), onlay position (OR = 0.224, 95%CI 0.095-0.524), and intraperitoneal position (OR = 0.564, 95%CI 0.366-0.869) was associated with a lower risk of incisional hernia compared to no mesh use. No statistically significant differences were observed in surgical site infection risk between the use of different mesh types or anatomical planes and no mesh placement.</p><p><strong>Conclusion: </strong>Prophylactic placement of prosthetic or bioprosthetic mesh in the retromuscular plane at the time of stoma closure is the most effective approach for reducing the incidence of incisional hernia and surgical site infection.</p>","PeriodicalId":13168,"journal":{"name":"Hernia","volume":"29 1","pages":"228"},"PeriodicalIF":2.4000,"publicationDate":"2025-07-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12241242/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hernia","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10029-025-03413-9","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Prophylactic mesh placement lowers incisional hernia risk, but the ideal mesh type and anatomical plane remain unclear. This study aims to determine which mesh and placement site are associated with the lowest rates of incisional hernia and surgical site infection after stoma closure.
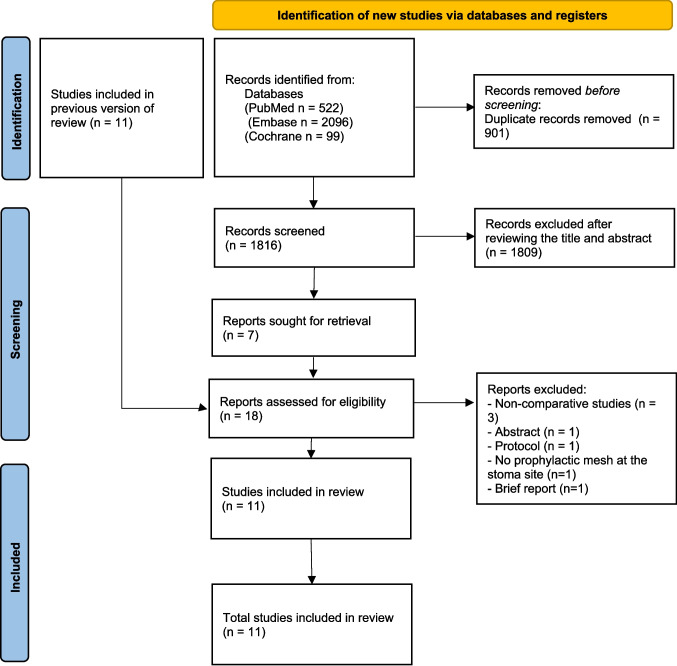
Methods: A systematic review of PubMed, the Cochrane Library, and Embase was conducted to identify comparative studies evaluating the type of mesh and/or the anatomical plane of mesh placement in the abdominal wall following stoma closure for the prevention of incisional hernias. A network meta-analysis was performed to assess incisional hernia and surgical site infection.
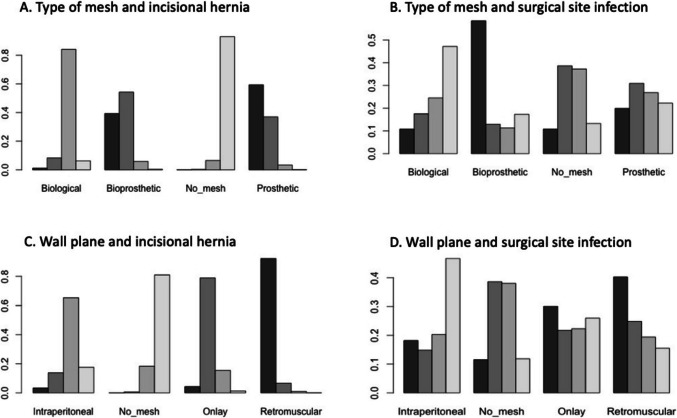
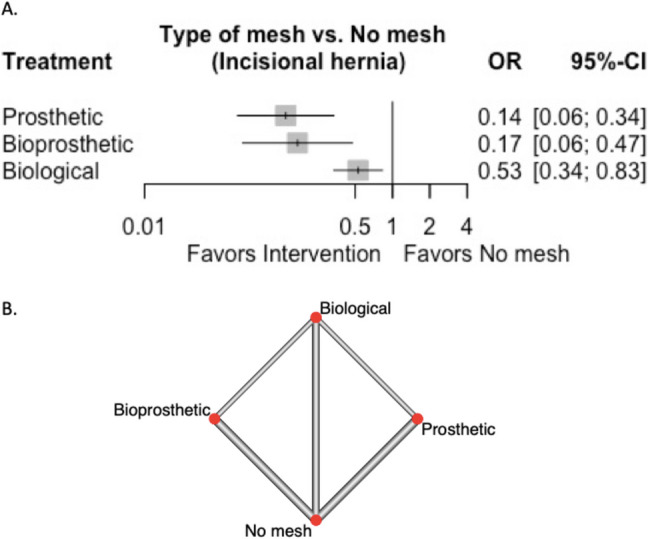
Results: We included 11 included studies involving 2,148 patients. The use of prosthetic mesh (OR = 0.137, 95%CI 0.056-0.335), bioprosthetic mesh (OR = 0.171, 95%CI 0.061-0.473), and biological mesh (OR = 0.528, 95%CI 0.336-0.828) was associated with a lower risk of incisional hernia compared to no mesh use. Mesh placement in a retromuscular position (OR = 0.068, 95%CI 0.024-0.189), onlay position (OR = 0.224, 95%CI 0.095-0.524), and intraperitoneal position (OR = 0.564, 95%CI 0.366-0.869) was associated with a lower risk of incisional hernia compared to no mesh use. No statistically significant differences were observed in surgical site infection risk between the use of different mesh types or anatomical planes and no mesh placement.
Conclusion: Prophylactic placement of prosthetic or bioprosthetic mesh in the retromuscular plane at the time of stoma closure is the most effective approach for reducing the incidence of incisional hernia and surgical site infection.
期刊介绍:
Hernia was founded in 1997 by Jean P. Chevrel with the purpose of promoting clinical studies and basic research as they apply to groin hernias and the abdominal wall . Since that time, a true revolution in the field of hernia studies has transformed the field from a ”simple” disease to one that is very specialized. While the majority of surgeries for primary inguinal and abdominal wall hernia are performed in hospitals worldwide, complex situations such as multi recurrences, complications, abdominal wall reconstructions and others are being studied and treated in specialist centers. As a result, major institutions and societies are creating specific parameters and criteria to better address the complexities of hernia surgery.
Hernia is a journal written by surgeons who have made abdominal wall surgery their specific field of interest, but we will consider publishing content from any surgeon who wishes to improve the science of this field. The Journal aims to ensure that hernia surgery is safer and easier for surgeons as well as patients, and provides a forum to all surgeons in the exchange of new ideas, results, and important research that is the basis of professional activity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


