Neoadjuvant triple-modality therapy with immune checkpoint blockade, anti-angiogenesis, and chemotherapy enhances pathologic response and survival in locally advanced and metastatic colorectal cancer: a multicenter cohort study.
Heng Wang, Junwei Zheng, Jun Pan, Shuliang Li, Bingbing Ren, Pei Wang, Bo Mo
{"title":"Neoadjuvant triple-modality therapy with immune checkpoint blockade, anti-angiogenesis, and chemotherapy enhances pathologic response and survival in locally advanced and metastatic colorectal cancer: a multicenter cohort study.","authors":"Heng Wang, Junwei Zheng, Jun Pan, Shuliang Li, Bingbing Ren, Pei Wang, Bo Mo","doi":"10.1007/s00384-025-04945-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The current study seeks to investigate the clinical outcomes of combining immune checkpoint blockade, anti-angiogenesis, and chemotherapy in neoadjuvant treatment for individuals diagnosed with locally advanced (high-risk Stage III or initially unresectable Stage III) or resectable/unresectable Stage IV colorectal cancer, including metastatic cases.</p><p><strong>Methods: </strong>A total of 120 individuals diagnosed with advanced colorectal cancer (stage III: n = 65; stage IV: n = 55; metastatic sites: liver n = 30, lung n = 15, peritoneal n = 10) were enrolled at three hospitals between February 2021 and December 2022. All patients underwent biopsy and pathology confirmation. Based on the treatment plan, patients were categorized into a control group (n = 60) receiving standard FOLFOX/FOLFIRI chemotherapy and an experimental group (n = 60) receiving a combination of pembrolizumab (200 mg IV q3w), bevacizumab (5 mg/kg IV q2w), and FOLFOX regimen (oxaliplatin 85 mg/m<sup>2</sup>, leucovorin 400 mg/m<sup>2</sup>, 5-fluorouracil 400 mg/m<sup>2</sup> bolus followed by 2400 mg/m<sup>2</sup> infusion over 46 h). VEGF and bFGF levels were assessed using ELISA before and after treatment. Flow cytometry analyzed CD4 + levels and the CD4 + /CD8 + ratio, while serum tumor markers Cancer antigen 199 (CA 19-9) and Carcinoembryonic antigen (CEA) were measured by chemiluminescence immunoassay. Therapeutic outcomes, median OS, and median PFS were compared between the two groups using Kaplan-Meier analysis and log-rank tests (normality confirmed via Shapiro-Wilk test).</p><p><strong>Results: </strong>After a 6-week treatment period, the experimental group showed a more significant reduction in VEGF (Δ = 132.0 pg/mL vs. 57.9 pg/mL) and bFGF (Δ = 51.4 pg/mL vs. 20.1 pg/mL) compared to the control group (P < 0.001). The experimental group demonstrated higher CD4 + /CD8 + ratios post-treatment (1.65 vs. 1.23, P < 0.01) and greater reductions in CA 19-9 (Δ = 42.5 U/mL vs. 23.8 U/mL) and CEA (Δ = 12.6 ng/mL vs. 6.9 ng/mL) (P < 0.01). Response rates (CR + PR: 40.0% (Experimental: 8.3% CR + 31.7% PR) vs. 18.4% (Control: 1.7% CR + 16.7% PR); DCR: 46.7% vs. 25.0%) and survival outcomes (median OS: 32.26 vs. 28.55 months; median PFS: 6.37 vs. 4.58 months) were superior in the experimental group (P < 0.05).</p><p><strong>Conclusion: </strong>Combining neoadjuvant therapy with immune checkpoint blockade, anti-angiogenesis, and chemotherapy significantly improves tumor downstaging (as evidenced by pathologic complete response rates of 18% in the experimental group vs. 5% in the control group among resected patients) and survival outcomes, presenting a promising therapeutic approach for locally advanced and oligometastatic colorectal cancer.</p>","PeriodicalId":13789,"journal":{"name":"International Journal of Colorectal Disease","volume":"40 1","pages":"154"},"PeriodicalIF":2.3000,"publicationDate":"2025-07-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12241296/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Colorectal Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00384-025-04945-3","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: The current study seeks to investigate the clinical outcomes of combining immune checkpoint blockade, anti-angiogenesis, and chemotherapy in neoadjuvant treatment for individuals diagnosed with locally advanced (high-risk Stage III or initially unresectable Stage III) or resectable/unresectable Stage IV colorectal cancer, including metastatic cases.
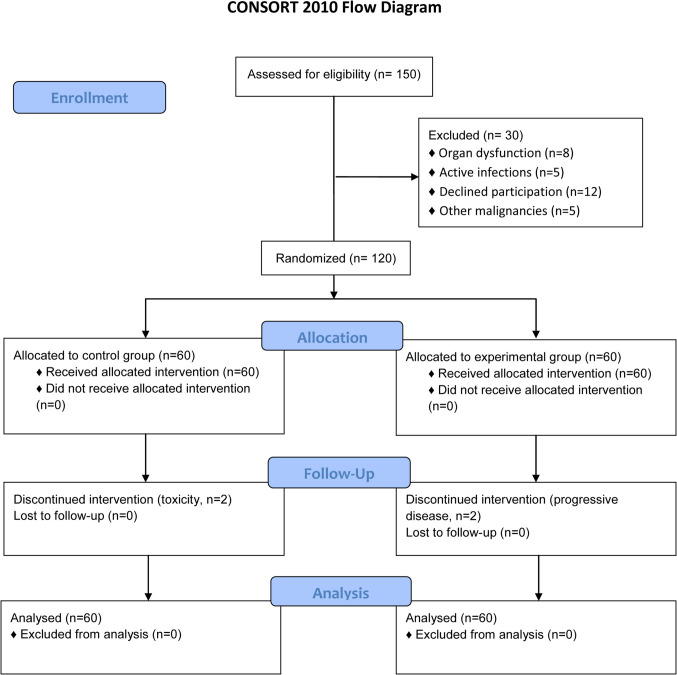
Methods: A total of 120 individuals diagnosed with advanced colorectal cancer (stage III: n = 65; stage IV: n = 55; metastatic sites: liver n = 30, lung n = 15, peritoneal n = 10) were enrolled at three hospitals between February 2021 and December 2022. All patients underwent biopsy and pathology confirmation. Based on the treatment plan, patients were categorized into a control group (n = 60) receiving standard FOLFOX/FOLFIRI chemotherapy and an experimental group (n = 60) receiving a combination of pembrolizumab (200 mg IV q3w), bevacizumab (5 mg/kg IV q2w), and FOLFOX regimen (oxaliplatin 85 mg/m2, leucovorin 400 mg/m2, 5-fluorouracil 400 mg/m2 bolus followed by 2400 mg/m2 infusion over 46 h). VEGF and bFGF levels were assessed using ELISA before and after treatment. Flow cytometry analyzed CD4 + levels and the CD4 + /CD8 + ratio, while serum tumor markers Cancer antigen 199 (CA 19-9) and Carcinoembryonic antigen (CEA) were measured by chemiluminescence immunoassay. Therapeutic outcomes, median OS, and median PFS were compared between the two groups using Kaplan-Meier analysis and log-rank tests (normality confirmed via Shapiro-Wilk test).
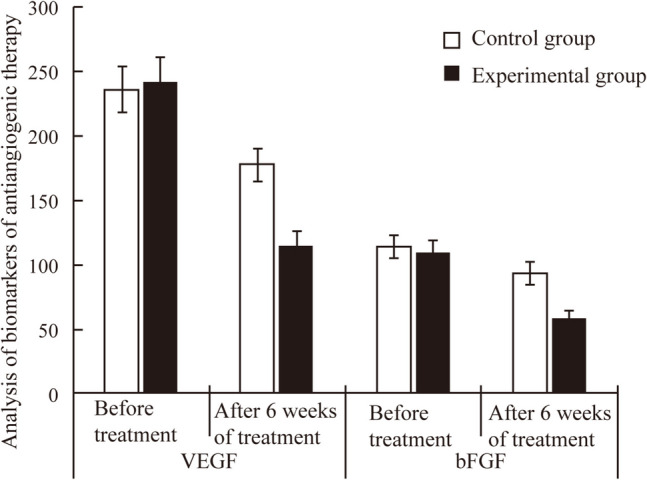
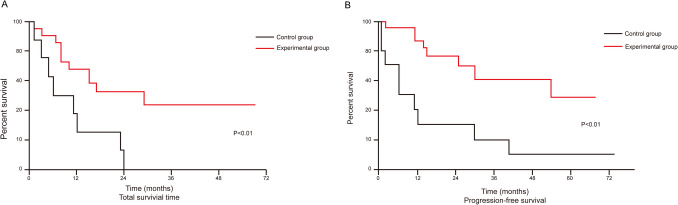
Results: After a 6-week treatment period, the experimental group showed a more significant reduction in VEGF (Δ = 132.0 pg/mL vs. 57.9 pg/mL) and bFGF (Δ = 51.4 pg/mL vs. 20.1 pg/mL) compared to the control group (P < 0.001). The experimental group demonstrated higher CD4 + /CD8 + ratios post-treatment (1.65 vs. 1.23, P < 0.01) and greater reductions in CA 19-9 (Δ = 42.5 U/mL vs. 23.8 U/mL) and CEA (Δ = 12.6 ng/mL vs. 6.9 ng/mL) (P < 0.01). Response rates (CR + PR: 40.0% (Experimental: 8.3% CR + 31.7% PR) vs. 18.4% (Control: 1.7% CR + 16.7% PR); DCR: 46.7% vs. 25.0%) and survival outcomes (median OS: 32.26 vs. 28.55 months; median PFS: 6.37 vs. 4.58 months) were superior in the experimental group (P < 0.05).
Conclusion: Combining neoadjuvant therapy with immune checkpoint blockade, anti-angiogenesis, and chemotherapy significantly improves tumor downstaging (as evidenced by pathologic complete response rates of 18% in the experimental group vs. 5% in the control group among resected patients) and survival outcomes, presenting a promising therapeutic approach for locally advanced and oligometastatic colorectal cancer.
期刊介绍:
The International Journal of Colorectal Disease, Clinical and Molecular Gastroenterology and Surgery aims to publish novel and state-of-the-art papers which deal with the physiology and pathophysiology of diseases involving the entire gastrointestinal tract. In addition to original research articles, the following categories will be included: reviews (usually commissioned but may also be submitted), case reports, letters to the editor, and protocols on clinical studies.
The journal offers its readers an interdisciplinary forum for clinical science and molecular research related to gastrointestinal disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


