Emma Rademaker, Daan F L Filippini, Jelle L G Haitsma Mulier, Marleen A Slim, Rombout B E van Amstel, Sivasubramanium V Bhavani, Nicole P Juffermans, Harm-Jan S de Grooth, Lennie P G Derde, Olaf L Cremer, Lieuwe D J Bos
{"title":"Immunobiological effects of tocilizumab across respiratory subphenotypes in COVID-19 ARDS.","authors":"Emma Rademaker, Daan F L Filippini, Jelle L G Haitsma Mulier, Marleen A Slim, Rombout B E van Amstel, Sivasubramanium V Bhavani, Nicole P Juffermans, Harm-Jan S de Grooth, Lennie P G Derde, Olaf L Cremer, Lieuwe D J Bos","doi":"10.1186/s40635-025-00779-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Two distinct longitudinal respiratory subphenotypes have recently been described in COVID-19-related acute respiratory distress syndrome (ARDS). These subphenotypes exhibit dynamic immunobiological changes that may help guide immunomodulatory interventions. However, the extent to which the immune response is determined by respiratory subphenotype in the presence of concurrent immunomodulatory treatment remains unclear. We investigated the independent and combined effects of respiratory subphenotype and tocilizumab on inflammatory response and clinical outcomes.</p><p><strong>Methods: </strong>We analyzed patients from existing COVID-19 biobanks who were consecutively admitted to the ICU and received more than 4 days of invasive mechanical ventilation between March 2020 and May 2022. Patients were classified into two previously described longitudinal respiratory subphenotypes-characterized by mechanical power, minute volume and ventilatory ratio-referred to as 'low-power' and 'high-power' subphenotypes. We analyzed how tocilizumab treatment and respiratory subphenotype were associated with endothelial and inflammatory plasma biomarkers on days 0, 4 and 7, as well as with mortality.</p><p><strong>Results: </strong>720 patients were included, of whom 464 (64%) and 256 (36%) were assigned to the low- and high-power subphenotypes, respectively. 108 (23%) of the low-power subphenotype patients received tocilizumab, and 43 (17%) of the high-power subphenotype. 427 patients had plasma samples available. The high-power subphenotype was associated with slightly higher SP-D, thrombomodulin and TNF-RI plasma concentrations on the day of intubation compared to the low-power subphenotype, along with a more rapid increase in IL-6 and TNF-RI levels in subjects who had received tocilizumab treatment (β = 0.14 log ng/ml, p = 0.022, and β = 0.06 log ng/ml, p = 0.014, respectively). Tocilizumab treatment accounted for four times more variance in IL-6 and angiopoietin-2 levels than subphenotype, while subphenotype explained only a small proportion of the variance and slightly more than tocilizumab for TNF-RI and thrombomodulin. Subphenotype did not modify the association between tocilizumab and mortality (IPTW adjusted hazard ratio 1.18; 95%CI 0.60-2.33).</p><p><strong>Conclusion: </strong>Respiratory subphenotypes showed varying TNF-RI and IL-6 responses to tocilizumab, but these differences were only minor compared to the drug's overall immunobiological effect. This suggests that respiratory subphenotype should not determine tocilizumab treatment decisions.</p>","PeriodicalId":13750,"journal":{"name":"Intensive Care Medicine Experimental","volume":"13 1","pages":"70"},"PeriodicalIF":2.8000,"publicationDate":"2025-07-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12240919/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Intensive Care Medicine Experimental","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40635-025-00779-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Two distinct longitudinal respiratory subphenotypes have recently been described in COVID-19-related acute respiratory distress syndrome (ARDS). These subphenotypes exhibit dynamic immunobiological changes that may help guide immunomodulatory interventions. However, the extent to which the immune response is determined by respiratory subphenotype in the presence of concurrent immunomodulatory treatment remains unclear. We investigated the independent and combined effects of respiratory subphenotype and tocilizumab on inflammatory response and clinical outcomes.
Methods: We analyzed patients from existing COVID-19 biobanks who were consecutively admitted to the ICU and received more than 4 days of invasive mechanical ventilation between March 2020 and May 2022. Patients were classified into two previously described longitudinal respiratory subphenotypes-characterized by mechanical power, minute volume and ventilatory ratio-referred to as 'low-power' and 'high-power' subphenotypes. We analyzed how tocilizumab treatment and respiratory subphenotype were associated with endothelial and inflammatory plasma biomarkers on days 0, 4 and 7, as well as with mortality.
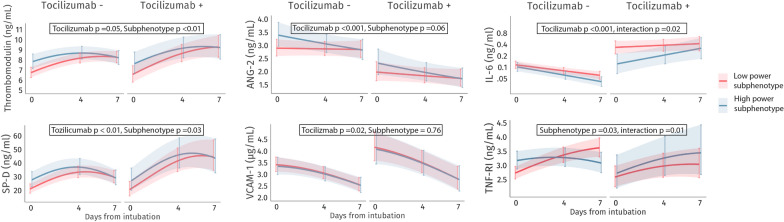
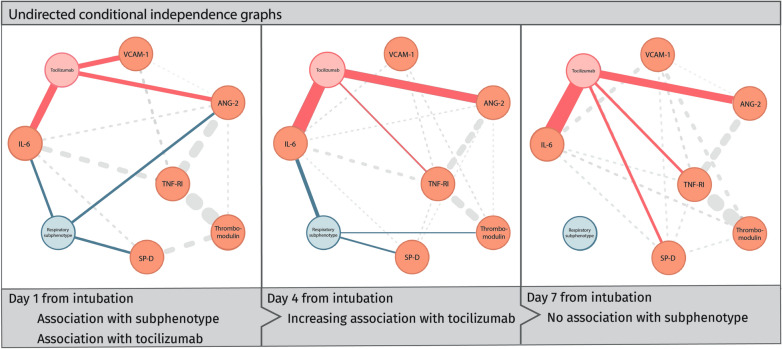
Results: 720 patients were included, of whom 464 (64%) and 256 (36%) were assigned to the low- and high-power subphenotypes, respectively. 108 (23%) of the low-power subphenotype patients received tocilizumab, and 43 (17%) of the high-power subphenotype. 427 patients had plasma samples available. The high-power subphenotype was associated with slightly higher SP-D, thrombomodulin and TNF-RI plasma concentrations on the day of intubation compared to the low-power subphenotype, along with a more rapid increase in IL-6 and TNF-RI levels in subjects who had received tocilizumab treatment (β = 0.14 log ng/ml, p = 0.022, and β = 0.06 log ng/ml, p = 0.014, respectively). Tocilizumab treatment accounted for four times more variance in IL-6 and angiopoietin-2 levels than subphenotype, while subphenotype explained only a small proportion of the variance and slightly more than tocilizumab for TNF-RI and thrombomodulin. Subphenotype did not modify the association between tocilizumab and mortality (IPTW adjusted hazard ratio 1.18; 95%CI 0.60-2.33).
Conclusion: Respiratory subphenotypes showed varying TNF-RI and IL-6 responses to tocilizumab, but these differences were only minor compared to the drug's overall immunobiological effect. This suggests that respiratory subphenotype should not determine tocilizumab treatment decisions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


