Brent M Troy, Maneesha Agarwal, Allison F Linden, Andrew Jergel, Anthony Giarusso, Kiesha Fraser Doh
{"title":"Child and neighborhood factors associated with pediatric injuries sustained while engaged in activities where helmet usage is recommended.","authors":"Brent M Troy, Maneesha Agarwal, Allison F Linden, Andrew Jergel, Anthony Giarusso, Kiesha Fraser Doh","doi":"10.1186/s40621-025-00598-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Unintentional injuries, including traumatic brain injuries (TBI) during activities where helmet usage is recommended (AWHUR), are a leading cause of pediatric morbidity and mortality in the U.S. While advocacy and education are proven measures to address safety, community resources in a child's neighborhood are known to have a large impact on their health.</p><p><strong>Methods: </strong>We utilized the trauma registry at two pediatric trauma centers, in a major metropolitan area from 2018 to 2022, to perform a retrospective chart review and Geographical Information System (GIS) mapping on all AWHUR injuries that were included in the trauma registry. Data extracted from the trauma registry included: mechanism, demographics, insurance status, and injury characteristics. AWHUR data was then overlaid with the Childhood Opportunity Index (COI) to assess community resources in relation to injury characteristics.</p><p><strong>Results: </strong>Our sample size included 1425 children throughout the 5-year time period. The most common injury mechanisms included: bicycle 34.0%, ATV 18.2%, skateboard 13.3%, scooter 9.2%, and dirt-bike 7.4%. Most patients in very low and low COI were publicly insured, respectively 81.9% and 63.2%; while 65.8% of high COI injured patients were privately insured children. There was a statistically significant difference in helmet usage across different levels of COI (p < 0.001). The rates of helmet usage by COI ranking from very low to very high were as follows: 21.6%, 25.2%, 37.8%, 40.2%, and 51.6% utilization. Among those injured while wearing a helmet, the odds of sustaining a higher ISS were 34% lower (OR = 0.66, 95% CI: 0.50-0.89) compared to those who were not wearing a helmet at the time of injury. Additionally, GIS mapping identified low and very low COI communities with higher injury rates and lower helmet use.</p><p><strong>Conclusion: </strong>Children with lower COI were more likely to be publicly insured with a lower percentage of helmet usage. Overlapping injury data and COI identified high-risk communities where low resources can contribute to growing injury severity. This data can then be used to inform injury prevention and highlight the importance of community factors.</p>","PeriodicalId":37379,"journal":{"name":"Injury Epidemiology","volume":"12 Suppl 1","pages":"39"},"PeriodicalIF":2.2000,"publicationDate":"2025-07-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12235759/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Injury Epidemiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40621-025-00598-6","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Unintentional injuries, including traumatic brain injuries (TBI) during activities where helmet usage is recommended (AWHUR), are a leading cause of pediatric morbidity and mortality in the U.S. While advocacy and education are proven measures to address safety, community resources in a child's neighborhood are known to have a large impact on their health.
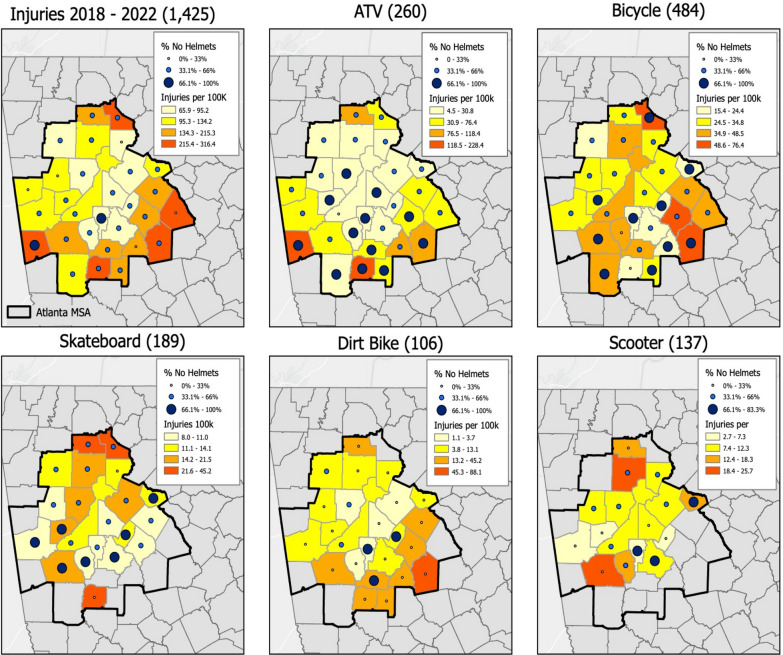
Methods: We utilized the trauma registry at two pediatric trauma centers, in a major metropolitan area from 2018 to 2022, to perform a retrospective chart review and Geographical Information System (GIS) mapping on all AWHUR injuries that were included in the trauma registry. Data extracted from the trauma registry included: mechanism, demographics, insurance status, and injury characteristics. AWHUR data was then overlaid with the Childhood Opportunity Index (COI) to assess community resources in relation to injury characteristics.
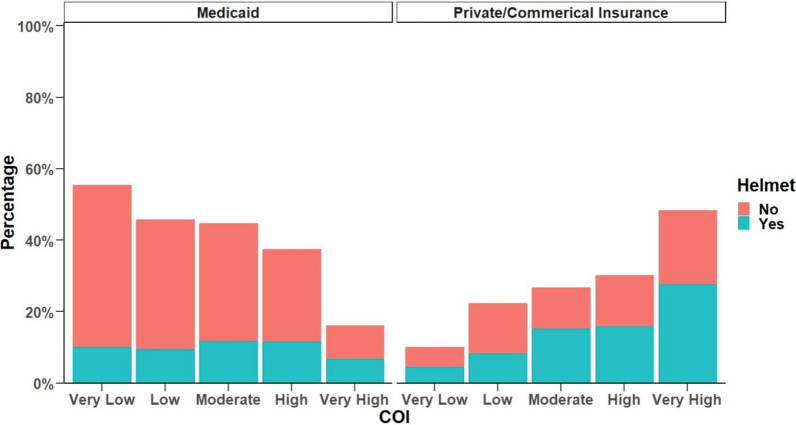
Results: Our sample size included 1425 children throughout the 5-year time period. The most common injury mechanisms included: bicycle 34.0%, ATV 18.2%, skateboard 13.3%, scooter 9.2%, and dirt-bike 7.4%. Most patients in very low and low COI were publicly insured, respectively 81.9% and 63.2%; while 65.8% of high COI injured patients were privately insured children. There was a statistically significant difference in helmet usage across different levels of COI (p < 0.001). The rates of helmet usage by COI ranking from very low to very high were as follows: 21.6%, 25.2%, 37.8%, 40.2%, and 51.6% utilization. Among those injured while wearing a helmet, the odds of sustaining a higher ISS were 34% lower (OR = 0.66, 95% CI: 0.50-0.89) compared to those who were not wearing a helmet at the time of injury. Additionally, GIS mapping identified low and very low COI communities with higher injury rates and lower helmet use.
Conclusion: Children with lower COI were more likely to be publicly insured with a lower percentage of helmet usage. Overlapping injury data and COI identified high-risk communities where low resources can contribute to growing injury severity. This data can then be used to inform injury prevention and highlight the importance of community factors.
期刊介绍:
Injury Epidemiology is dedicated to advancing the scientific foundation for injury prevention and control through timely publication and dissemination of peer-reviewed research. Injury Epidemiology aims to be the premier venue for communicating epidemiologic studies of unintentional and intentional injuries, including, but not limited to, morbidity and mortality from motor vehicle crashes, drug overdose/poisoning, falls, drowning, fires/burns, iatrogenic injury, suicide, homicide, assaults, and abuse. We welcome investigations designed to understand the magnitude, distribution, determinants, causes, prevention, diagnosis, treatment, prognosis, and outcomes of injuries in specific population groups, geographic regions, and environmental settings (e.g., home, workplace, transport, recreation, sports, and urban/rural). Injury Epidemiology has a special focus on studies generating objective and practical knowledge that can be translated into interventions to reduce injury morbidity and mortality on a population level. Priority consideration will be given to manuscripts that feature contemporary theories and concepts, innovative methods, and novel techniques as applied to injury surveillance, risk assessment, development and implementation of effective interventions, and program and policy evaluation.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


