Analysis of frailty change trajectories and its risk factors in patients with gastrointestinal tumor surgery: a prospective observational longitudinal study.
{"title":"Analysis of frailty change trajectories and its risk factors in patients with gastrointestinal tumor surgery: a prospective observational longitudinal study.","authors":"Junli You, Xiaohong Lv, Yu Rong, Xuepiao Chen, Tianxiao Liu, Yubo Xie","doi":"10.1186/s12957-025-03924-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Frailty is a dynamic process, but its changes following surgery are unclear. This study aimed to investigate frailty change trajectories and their risk factors in older patients undergoing gastrointestinal tumor surgery.</p><p><strong>Methods: </strong>The Frail Scale (FS) assessed frailty from preoperative to 180 days after surgery. The latent class analysis (LCA) was established to identify the most fitting latent class, and the risk factors of these change trajectories were analyzed. We also recorded and explored changes in FS components.</p><p><strong>Results: </strong>212 elderly patients (aged ≥ 60 years) scheduled for gastrointestinal tumor surgery under general anesthesia completed the study. The LCA identified four optimal trajectory groups. There are differences in gender, age, marriage, American Society of Anesthesiologists (ASA) classification, number of comorbidities, hemoglobin, Charlson comorbidity index (CCI), the six-minute walk test (6MWT), metabolic equivalent (MET), preoperative frailty status, and time to first ambulation among the four groups (P < 0.05). Comorbidities, MET, preoperative frailty, age, first time to ambulation, and 6WMT were independent factors influencing abnormal frailty trajectories. Overall, the FS components all changed 180 days after the surgery. Except for weight loss, the changes in the other components were related to the surgical site (P < 0.05).</p><p><strong>Conclusion: </strong>Frailty is a dynamic process. Older patients with more comorbidities, low MET and 6WMT, preoperative frailty, and later time to ambulation are prone to remain in frailty or transition to it after surgery. Clinical attention and targeted rehabilitation should be provided to them.</p>","PeriodicalId":23856,"journal":{"name":"World Journal of Surgical Oncology","volume":"23 1","pages":"264"},"PeriodicalIF":2.5000,"publicationDate":"2025-07-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12235829/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Surgical Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12957-025-03924-w","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Frailty is a dynamic process, but its changes following surgery are unclear. This study aimed to investigate frailty change trajectories and their risk factors in older patients undergoing gastrointestinal tumor surgery.
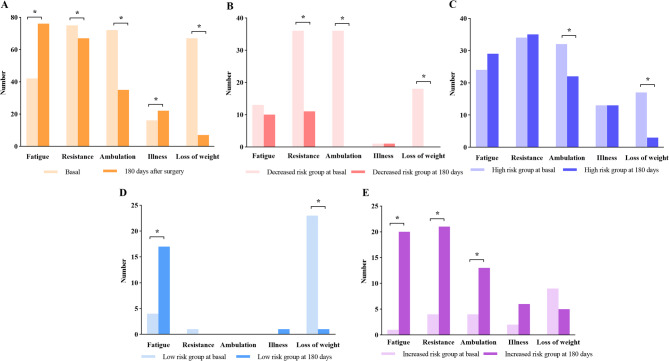
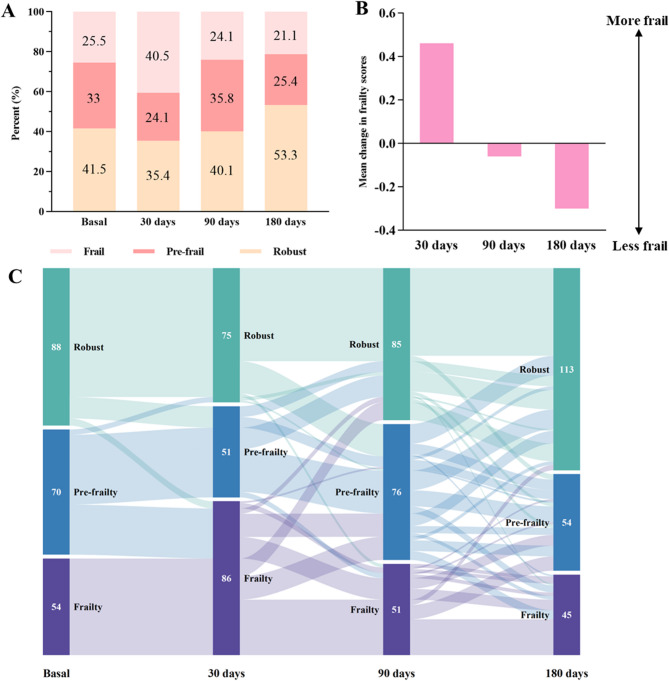
Methods: The Frail Scale (FS) assessed frailty from preoperative to 180 days after surgery. The latent class analysis (LCA) was established to identify the most fitting latent class, and the risk factors of these change trajectories were analyzed. We also recorded and explored changes in FS components.
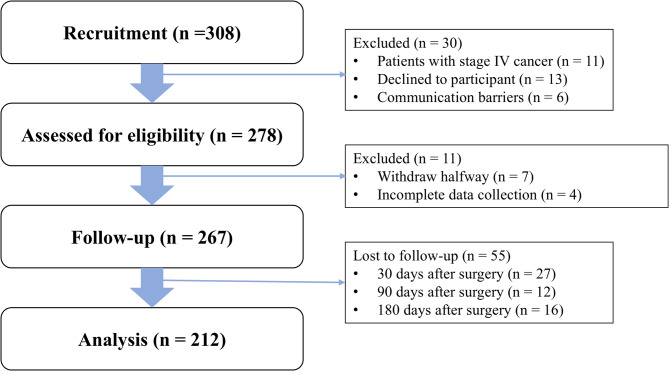
Results: 212 elderly patients (aged ≥ 60 years) scheduled for gastrointestinal tumor surgery under general anesthesia completed the study. The LCA identified four optimal trajectory groups. There are differences in gender, age, marriage, American Society of Anesthesiologists (ASA) classification, number of comorbidities, hemoglobin, Charlson comorbidity index (CCI), the six-minute walk test (6MWT), metabolic equivalent (MET), preoperative frailty status, and time to first ambulation among the four groups (P < 0.05). Comorbidities, MET, preoperative frailty, age, first time to ambulation, and 6WMT were independent factors influencing abnormal frailty trajectories. Overall, the FS components all changed 180 days after the surgery. Except for weight loss, the changes in the other components were related to the surgical site (P < 0.05).
Conclusion: Frailty is a dynamic process. Older patients with more comorbidities, low MET and 6WMT, preoperative frailty, and later time to ambulation are prone to remain in frailty or transition to it after surgery. Clinical attention and targeted rehabilitation should be provided to them.
期刊介绍:
World Journal of Surgical Oncology publishes articles related to surgical oncology and its allied subjects, such as epidemiology, cancer research, biomarkers, prevention, pathology, radiology, cancer treatment, clinical trials, multimodality treatment and molecular biology. Emphasis is placed on original research articles. The journal also publishes significant clinical case reports, as well as balanced and timely reviews on selected topics.
Oncology is a multidisciplinary super-speciality of which surgical oncology forms an integral component, especially with solid tumors. Surgical oncologists around the world are involved in research extending from detecting the mechanisms underlying the causation of cancer, to its treatment and prevention. The role of a surgical oncologist extends across the whole continuum of care. With continued developments in diagnosis and treatment, the role of a surgical oncologist is ever-changing. Hence, World Journal of Surgical Oncology aims to keep readers abreast with latest developments that will ultimately influence the work of surgical oncologists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


