{"title":"Development and validation of a nomogram prediction model for surgical site infection after instrumentation for degenerative lumbar spinal diseases.","authors":"Yongjun Liu, Xiaodong Wei, Xiaoyan Chen, Yan Ding","doi":"10.1186/s13741-025-00556-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This retrospective study aimed to investigate the incidence and risk factors for surgical site infection (SSI) following instrumentation for degenerative lumbar spinal diseases, and to develop a predictive nomogram model.</p><p><strong>Method: </strong>Patients who underwent posterior instrumentation for degenerative lumbar spinal diseases between January 2020 and December 2022 with a minimum 12-month follow-up were included. Patients were classified as having an SSI or not, and differences in demographics, clinical data, and laboratory indicators were compared. Multivariate logistic regression was performed to identify independent risk factors, and a nomogram was constructed to visualize the results.</p><p><strong>Results: </strong>The study included 1,462 patients (687 men, 775 women) with a mean age of 52.9 ± 13.7 years and 53 patients (3.5%) developed an SSI. Multivariate analysis identified several risk factors for SSI: higher ASA class (III or IV vs I or II, OR = 2.362; 95%CI, 1.312 to 4.249), surgery involving sacral vertebrae (OR = 2.319; 95%CI, 1.242 to 4.330), open surgery compared to minimally invasive surgery (OR = 3.081; 95%CI, 1.701 to 5.581), prolonged surgical time (per hour increase, OR = 1.482; 95%CI, 1.017 to 2.160), and preoperative hemoglobin < 100 g/L (OR = 4.962; 95%CI, 1.728 to 6.943). The nomogram model demonstrated good discrimination, with a C-index of 0.743 (95% CI: 0.682-0.804), which remained robust at 0.722 after 1,000 bootstrap verifications. The calibration curve indicated the predicted SSI probability aligned well with the actual probability.</p><p><strong>Conclusions: </strong>This study found a moderate 3.5% SSI rate following instrumentation for degenerative lumbar spinal diseases and identified several risk factors. These findings can inform preoperative patient counseling, risk assessment, and the development of personalized strategies to mitigate SSI.</p>","PeriodicalId":19764,"journal":{"name":"Perioperative Medicine","volume":"14 1","pages":"71"},"PeriodicalIF":2.1000,"publicationDate":"2025-07-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12235930/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Perioperative Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13741-025-00556-2","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: This retrospective study aimed to investigate the incidence and risk factors for surgical site infection (SSI) following instrumentation for degenerative lumbar spinal diseases, and to develop a predictive nomogram model.
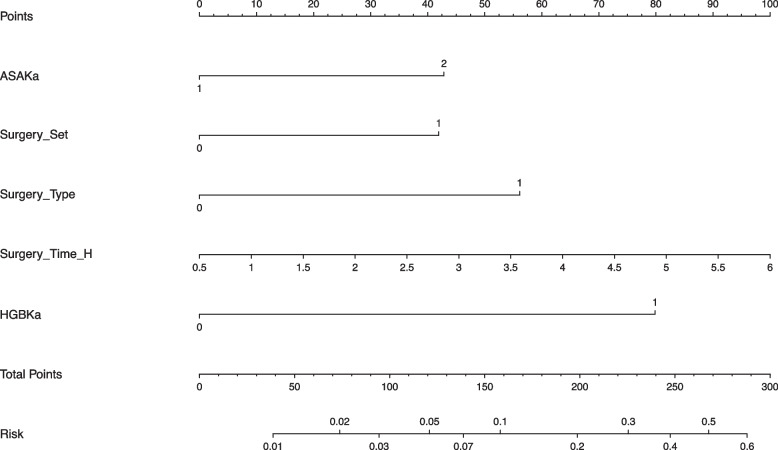
Method: Patients who underwent posterior instrumentation for degenerative lumbar spinal diseases between January 2020 and December 2022 with a minimum 12-month follow-up were included. Patients were classified as having an SSI or not, and differences in demographics, clinical data, and laboratory indicators were compared. Multivariate logistic regression was performed to identify independent risk factors, and a nomogram was constructed to visualize the results.
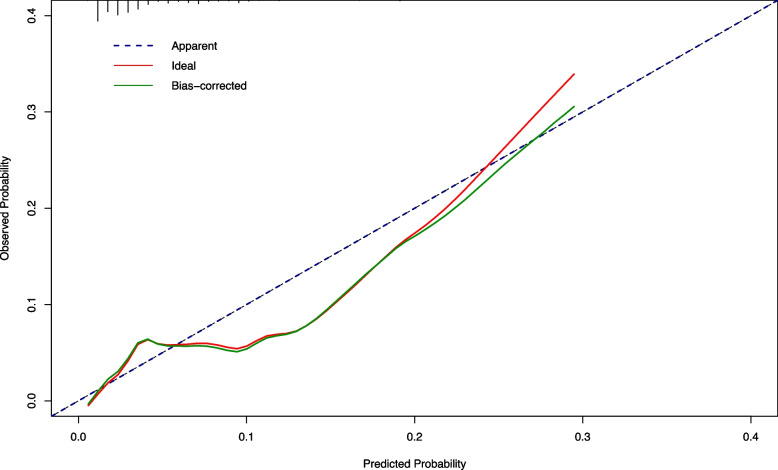
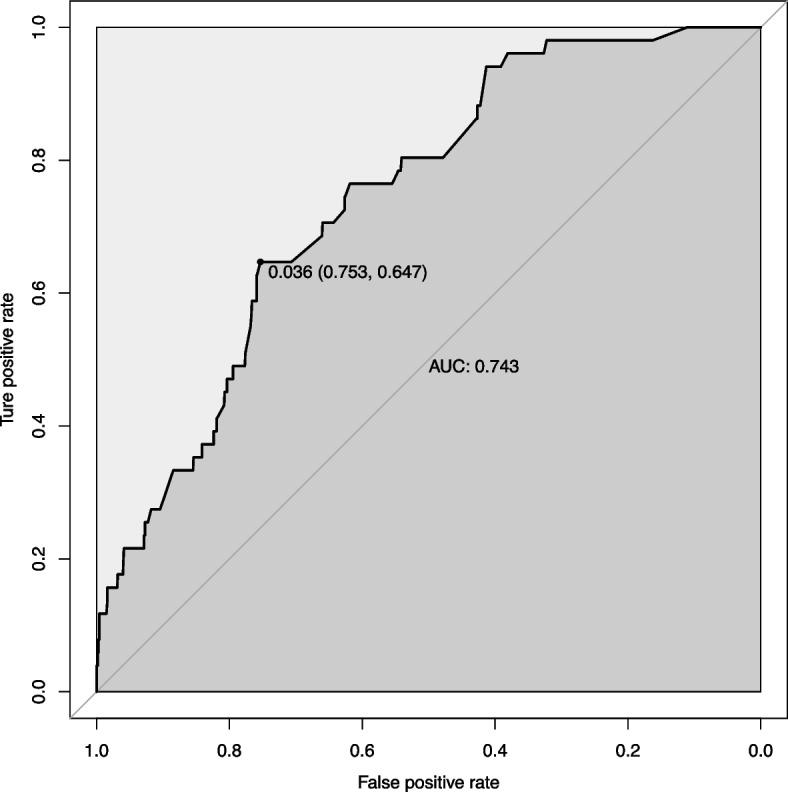
Results: The study included 1,462 patients (687 men, 775 women) with a mean age of 52.9 ± 13.7 years and 53 patients (3.5%) developed an SSI. Multivariate analysis identified several risk factors for SSI: higher ASA class (III or IV vs I or II, OR = 2.362; 95%CI, 1.312 to 4.249), surgery involving sacral vertebrae (OR = 2.319; 95%CI, 1.242 to 4.330), open surgery compared to minimally invasive surgery (OR = 3.081; 95%CI, 1.701 to 5.581), prolonged surgical time (per hour increase, OR = 1.482; 95%CI, 1.017 to 2.160), and preoperative hemoglobin < 100 g/L (OR = 4.962; 95%CI, 1.728 to 6.943). The nomogram model demonstrated good discrimination, with a C-index of 0.743 (95% CI: 0.682-0.804), which remained robust at 0.722 after 1,000 bootstrap verifications. The calibration curve indicated the predicted SSI probability aligned well with the actual probability.
Conclusions: This study found a moderate 3.5% SSI rate following instrumentation for degenerative lumbar spinal diseases and identified several risk factors. These findings can inform preoperative patient counseling, risk assessment, and the development of personalized strategies to mitigate SSI.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


