Alejandro Avello, Raúl Fernández-Prado, Daria Abasheva, Ignacio Mahillo, Miguel Ángel González-Gay, Catalina Martín-Cleary, José Miguel Arce-Obieta, María Vanessa Pérez-Gómez, Beatriz Fernández-Fernández, Alberto Ortiz
{"title":"Heterogeneity of regional and national hospitalization burden of lupus nephritis and systemic lupus erythematous.","authors":"Alejandro Avello, Raúl Fernández-Prado, Daria Abasheva, Ignacio Mahillo, Miguel Ángel González-Gay, Catalina Martín-Cleary, José Miguel Arce-Obieta, María Vanessa Pérez-Gómez, Beatriz Fernández-Fernández, Alberto Ortiz","doi":"10.1093/ckj/sfaf162","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Differences between regional healthcare systems in the in-hospital burden and care of systemic lupus erythematosus (SLE) and lupus nephritis (LN) are poorly characterized. Their analysis may provide benchmarking opportunities that improve the quality and sustainability of care.</p><p><strong>Methods: </strong>We retrospectively investigated the hospitalization burden of SLE and LN in 2019-2021 across Spanish regional healthcare systems using the Spanish National Hospital Discharge Records database (RAE-CMBD) and National Statistics Institute (INE) data.</p><p><strong>Results: </strong>Of 66 262 724 hospitalization episodes from 644 public and private hospitals, 10 781 had a primary diagnosis of SLE, of which 2481 (23%) were for LN. The mean annual nationwide hospitalization case incidence was 70.61 and 1.75 per 100 000 population for SLE and LN, respectively. Regional differences were large: 48.0-fold and 6.9-fold between regions with the highest and lowest incidence for SLE and LN, respectively. In multivariate analysis, net household income and percentage of foreign-born population were associated with the number of SLE and LN hospitalization episodes. Internal medicine managed 28% of SLE and 15% of LN hospitalizations, nephrology 14% and 56% and rheumatology 23% and 11%, respectively, but there were large regional differences. The mean SLE and LN stays were 8.85 and 6.92 days (5.47 and 5.41 for nephrology and 11.18 and 11.83 for internal medicine), respectively. The average all patient refined diagnosis related groups (APR-DRGs) cost per episode was €2408 for SLE and €3563 for LN. The average yearly costs were €167 985 per million population (pmp) for SLE hospitalizations (4.32-fold differences between regions) and €60 825 pmp for LN hospitalizations (4.20-fold differences between regions). Large differences between regions were observed in the cost burden pmp relative to household income (4.70-fold for LN and 4.13-fold for SLE).</p><p><strong>Conclusion: </strong>In real-world clinical practice, the burden of in-hospital care of LN and SLE is heterogeneous across and within regional healthcare systems, offering the opportunity to benchmark best practice, optimize care and improve outcomes.</p>","PeriodicalId":10435,"journal":{"name":"Clinical Kidney Journal","volume":"18 7","pages":"sfaf162"},"PeriodicalIF":4.6000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12230550/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Kidney Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ckj/sfaf162","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Differences between regional healthcare systems in the in-hospital burden and care of systemic lupus erythematosus (SLE) and lupus nephritis (LN) are poorly characterized. Their analysis may provide benchmarking opportunities that improve the quality and sustainability of care.
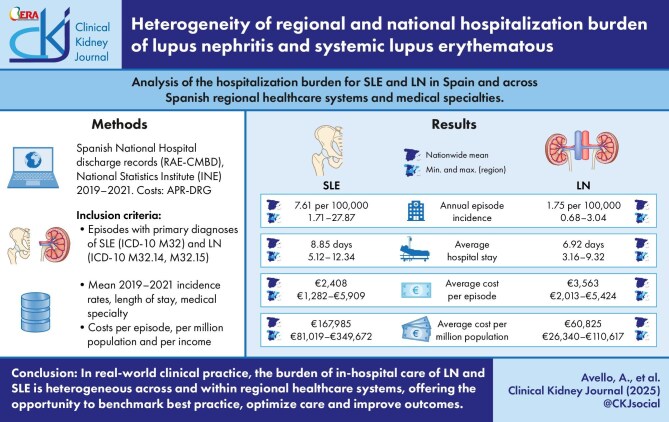
Methods: We retrospectively investigated the hospitalization burden of SLE and LN in 2019-2021 across Spanish regional healthcare systems using the Spanish National Hospital Discharge Records database (RAE-CMBD) and National Statistics Institute (INE) data.
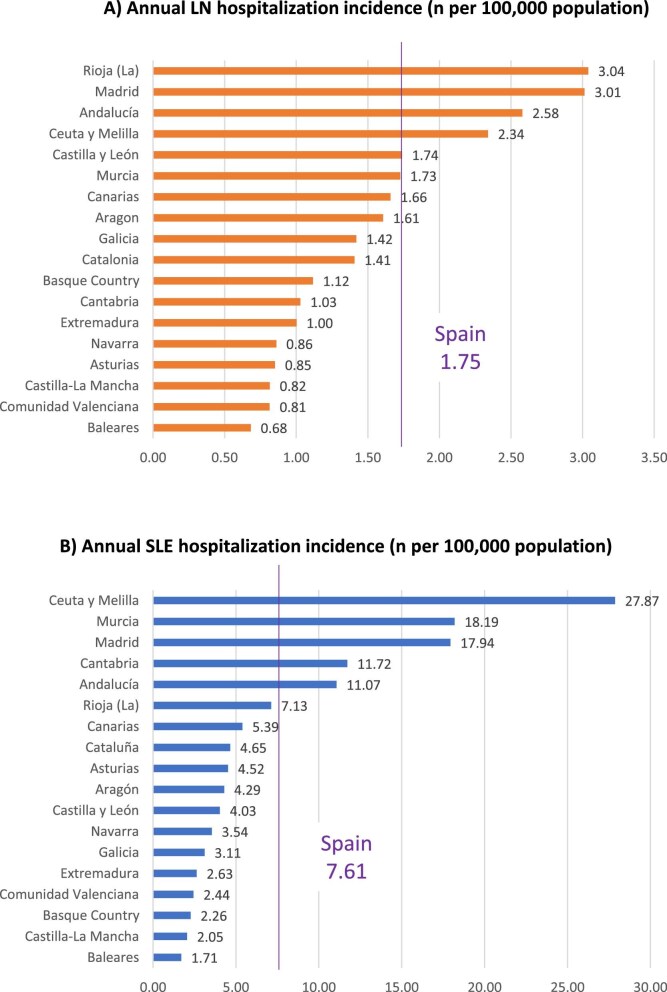
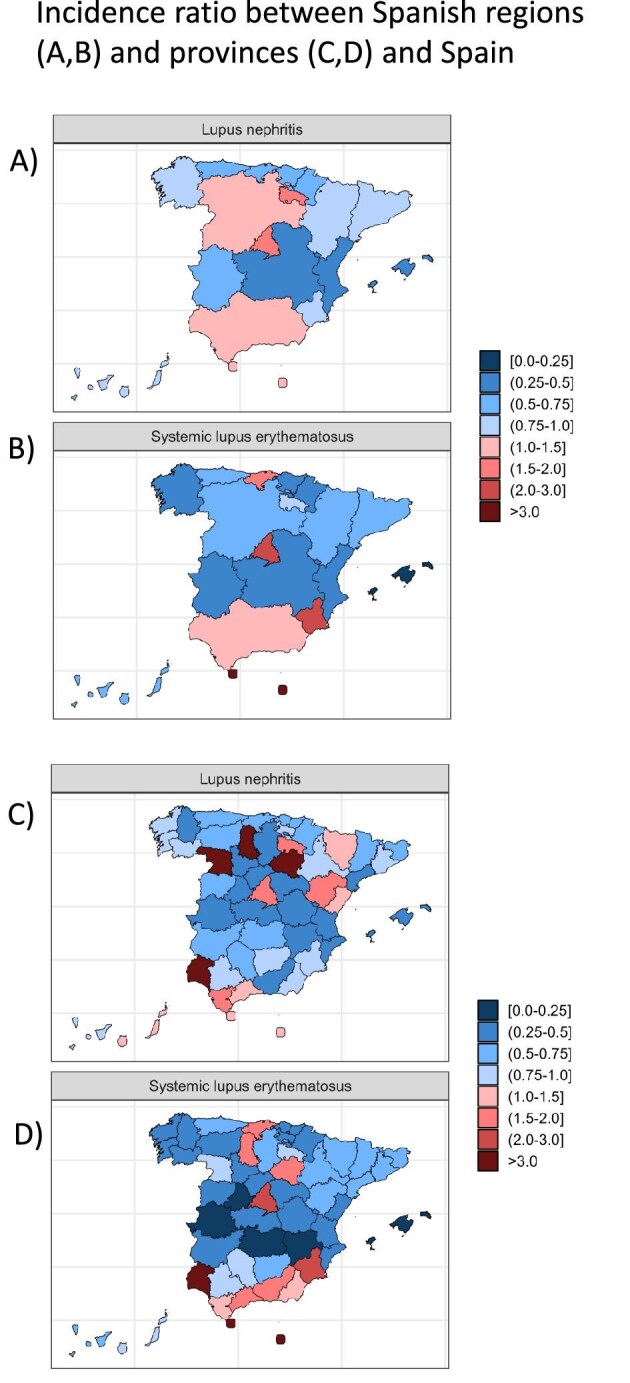
Results: Of 66 262 724 hospitalization episodes from 644 public and private hospitals, 10 781 had a primary diagnosis of SLE, of which 2481 (23%) were for LN. The mean annual nationwide hospitalization case incidence was 70.61 and 1.75 per 100 000 population for SLE and LN, respectively. Regional differences were large: 48.0-fold and 6.9-fold between regions with the highest and lowest incidence for SLE and LN, respectively. In multivariate analysis, net household income and percentage of foreign-born population were associated with the number of SLE and LN hospitalization episodes. Internal medicine managed 28% of SLE and 15% of LN hospitalizations, nephrology 14% and 56% and rheumatology 23% and 11%, respectively, but there were large regional differences. The mean SLE and LN stays were 8.85 and 6.92 days (5.47 and 5.41 for nephrology and 11.18 and 11.83 for internal medicine), respectively. The average all patient refined diagnosis related groups (APR-DRGs) cost per episode was €2408 for SLE and €3563 for LN. The average yearly costs were €167 985 per million population (pmp) for SLE hospitalizations (4.32-fold differences between regions) and €60 825 pmp for LN hospitalizations (4.20-fold differences between regions). Large differences between regions were observed in the cost burden pmp relative to household income (4.70-fold for LN and 4.13-fold for SLE).
Conclusion: In real-world clinical practice, the burden of in-hospital care of LN and SLE is heterogeneous across and within regional healthcare systems, offering the opportunity to benchmark best practice, optimize care and improve outcomes.
期刊介绍:
About the Journal
Clinical Kidney Journal: Clinical and Translational Nephrology (ckj), an official journal of the ERA-EDTA (European Renal Association-European Dialysis and Transplant Association), is a fully open access, online only journal publishing bimonthly. The journal is an essential educational and training resource integrating clinical, translational and educational research into clinical practice. ckj aims to contribute to a translational research culture among nephrologists and kidney pathologists that helps close the gap between basic researchers and practicing clinicians and promote sorely needed innovation in the Nephrology field. All research articles in this journal have undergone peer review.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


