Association between preexisting long-term care needs and in-hospital mortality and long-term outcomes in older inpatients with pneumonia: A retrospective cohort study
{"title":"Association between preexisting long-term care needs and in-hospital mortality and long-term outcomes in older inpatients with pneumonia: A retrospective cohort study","authors":"Jumpei Taniguchi MD, Hayato Yamana MD, PhD, Yuichiro Matsuo MD, Yusuke Sasabuchi MD, PhD, Hiroki Matsui PhD, Takahide Kohro MD, PhD, Hideo Yasunaga MD, PhD","doi":"10.1002/jgf2.70016","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Limited evidence exists regarding the impact of baseline functional and cognitive impairments on the outcomes of patients with pneumonia.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We used medical and long-term care administrative databases in a prefecture in Japan that contained care need levels assessed using the national standardized certification system. We identified patients aged ≥65 years who were hospitalized for pneumonia between June 2014 and October 2018. The impairments were classified into four categories based on estimated total daily care time: no care needs, support levels 1–2, care needs level 1 (estimated care time of 25–49 min), care needs level 2–3 (50–89 min), and care needs level 4–5 (≥90 min). The primary outcome was the in-hospital mortality rate. Secondary outcomes were death and care needs at 6 months and 1 year after admission. We evaluated the outcomes based on care need levels and conducted multivariate analyses adjusting for potential confounders.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 15,537 patients (mean age 83.9 years) were included. The in-hospital mortality rates for patients with no care needs, support levels 1–2 and care needs level 1, care needs levels 2–3, and care needs levels 4–5 were 10.5%, 15.9%, 21.1%, and 24.7%, respectively. The proportions of patients who died or experienced worsening care needs at 6 months were 43.6%, 60.4%, 60.0%, and 50.2%, respectively. Multivariable analyses demonstrated independent associations of preexisting care needs with both in-hospital mortality and long-term outcomes.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Preexisting long-term care needs are associated with short- and long-term outcomes in older inpatients with pneumonia.</p>\n </section>\n </div>","PeriodicalId":51861,"journal":{"name":"Journal of General and Family Medicine","volume":"26 4","pages":"326-333"},"PeriodicalIF":2.3000,"publicationDate":"2025-04-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jgf2.70016","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of General and Family Medicine","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jgf2.70016","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Limited evidence exists regarding the impact of baseline functional and cognitive impairments on the outcomes of patients with pneumonia.
Methods
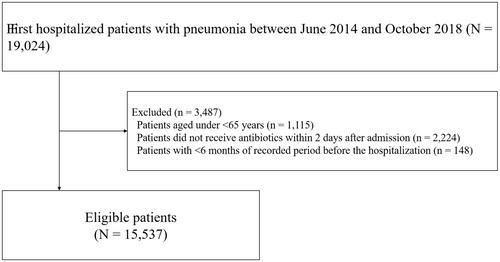
We used medical and long-term care administrative databases in a prefecture in Japan that contained care need levels assessed using the national standardized certification system. We identified patients aged ≥65 years who were hospitalized for pneumonia between June 2014 and October 2018. The impairments were classified into four categories based on estimated total daily care time: no care needs, support levels 1–2, care needs level 1 (estimated care time of 25–49 min), care needs level 2–3 (50–89 min), and care needs level 4–5 (≥90 min). The primary outcome was the in-hospital mortality rate. Secondary outcomes were death and care needs at 6 months and 1 year after admission. We evaluated the outcomes based on care need levels and conducted multivariate analyses adjusting for potential confounders.
Results
A total of 15,537 patients (mean age 83.9 years) were included. The in-hospital mortality rates for patients with no care needs, support levels 1–2 and care needs level 1, care needs levels 2–3, and care needs levels 4–5 were 10.5%, 15.9%, 21.1%, and 24.7%, respectively. The proportions of patients who died or experienced worsening care needs at 6 months were 43.6%, 60.4%, 60.0%, and 50.2%, respectively. Multivariable analyses demonstrated independent associations of preexisting care needs with both in-hospital mortality and long-term outcomes.
Conclusion
Preexisting long-term care needs are associated with short- and long-term outcomes in older inpatients with pneumonia.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


