Association Between Albumin Corrected Anion Gap and 28-Day All-Cause Mortality in Patients With Acute Respiratory Failure in ICU: A Retrospective Study Based on the MIMIC-IV Database
Abstract
Background
For critically ill patients in the intensive care unit (ICU), acute respiratory failure (ARF) stands as a prominent cause of mortality. Anion gap (AG) denotes the disparity between unmeasured cations and anions. Adjusting AG for albumin levels results in the albumin corrected anion gap (ACAG), which provides a more accurate representation of the body's acid–base status. Elevated ACAG may arise from ARF-induced cellular hypoxia and metabolic acidosis. However, limited research has investigated the association between ACAG and the 28-day all-cause mortality of ARF patients in critical care.
Methods
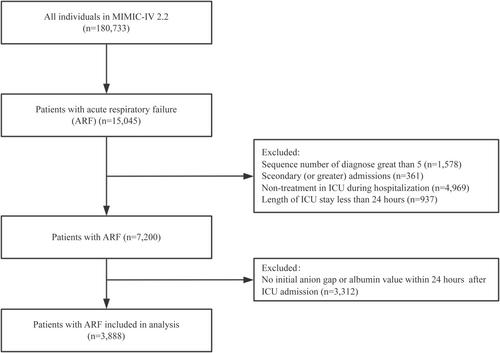
Using the Medical Information Mart for Intensive Care (MIMIC-IV 2.2) database, a retrospective data analysis was conducted, specifically targeting critically ill patients diagnosed with ARF. Serum ACAG was collected within 24 hours of the patient's admission to the ICU. The association between ACAG levels and 28-day all-cause mortality was investigated using smooth curve fitting, a multivariate Cox proportional hazard regression model, and Kaplan–Meier survival curve analysis. Furthermore, the consistency of these relationships was assessed through interaction and subgroup analyses.
Results
The study involved the enrollment of 3888 eligible participants in total. After adjusting for confounding variables in the multivariable Cox regression analysis model, we noticed a positive linear relationship between the ACAG value and the ICU's 28-day all-cause mortality rate. When ACAG was used as a continuous variable, a 3.1% increase in 28-day all-cause mortality was associated with a 1.0-mmol/L increase in ACAG (adjusted HR = 1.037, 95% CI: 1.025–1.048, p < 0.001). In the 28-day all-cause mortality, the highest and intermediate ACAG groups (adjusted HR 1.483, 95% CI: 1.244–1.768 and adjusted HR 1.244, 95% CI: 1.062–1.457, respectively) were notably higher than the lowest ACAG group when ACAG was utilized as a tertiles categorical variable. The substantial association between ACAG and 28-day all-cause mortality in the ICU was consistently demonstrated through subgroup analysis.
Conclusions
Among ICU patients with ARF, an elevated ACAG is linked to an elevated risk of 28-day all-cause mortality. There exists a linearly positive relationship between the 28-day all-cause mortality and ACAG.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


