Till Wagner, Marloes Nienhuijs, Stefaan Berge, Dietmar Ulrich
{"title":"Z-back-cut cheiloplasty: a cadaveric and clinical study on lip lengthening in unilateral cleft lip repair as a proof of concept.","authors":"Till Wagner, Marloes Nienhuijs, Stefaan Berge, Dietmar Ulrich","doi":"10.1186/s40902-025-00470-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The clinical outcome of unilateral cleft lip closure depends on both the incision pattern and vertical scar retraction as well as complete lip muscle closure. Existing techniques focus on the lengthening of the cleft side with reducing visible scarring in addition to correct muscle adaptation but are still struggling with scar contraction. We aimed to optimize clinical results by developing a new incision design integrating benefits of established techniques with our own considerations.</p><p><strong>Methods: </strong>A study-using 10 adult cadavers-compared two vertical incision lines: the Millard advancement-rotation flap and our Z-back-cut cheiloplasty which reassembles a Z-plasty at the nostril by combining with a back cut at the lower columella rim. A skin distraction model assessed the impact of tension on lengthening. Our technique demonstrated increased vertical height compared to Millard's method. Based on these findings, we applied our approach in clinical settings.</p><p><strong>Results: </strong>The Millard flap showed significantly less elongation (up to 35%) between the lateral cupid's bow and the columella base than our method. This suggests that the Z-plasty principle is beneficial in unilateral cleft lip closure. Clinical outcomes confirmed its applicability in both partial and complete clefts.</p><p><strong>Discussion: </strong>Applying our findings in pediatric patients yielded at least equivalent results to the Millard II technique, even in cases with postoperative wound infections and increased contraction risk.</p><p><strong>Conclusion: </strong>Our research supports integrating Z-plasty principles into unilateral cleft lip repair. We plan to use this technique in future surgeries where indicated.</p>","PeriodicalId":18357,"journal":{"name":"Maxillofacial Plastic and Reconstructive Surgery","volume":"47 1","pages":"16"},"PeriodicalIF":2.8000,"publicationDate":"2025-07-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12234926/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Maxillofacial Plastic and Reconstructive Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40902-025-00470-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"DENTISTRY, ORAL SURGERY & MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The clinical outcome of unilateral cleft lip closure depends on both the incision pattern and vertical scar retraction as well as complete lip muscle closure. Existing techniques focus on the lengthening of the cleft side with reducing visible scarring in addition to correct muscle adaptation but are still struggling with scar contraction. We aimed to optimize clinical results by developing a new incision design integrating benefits of established techniques with our own considerations.
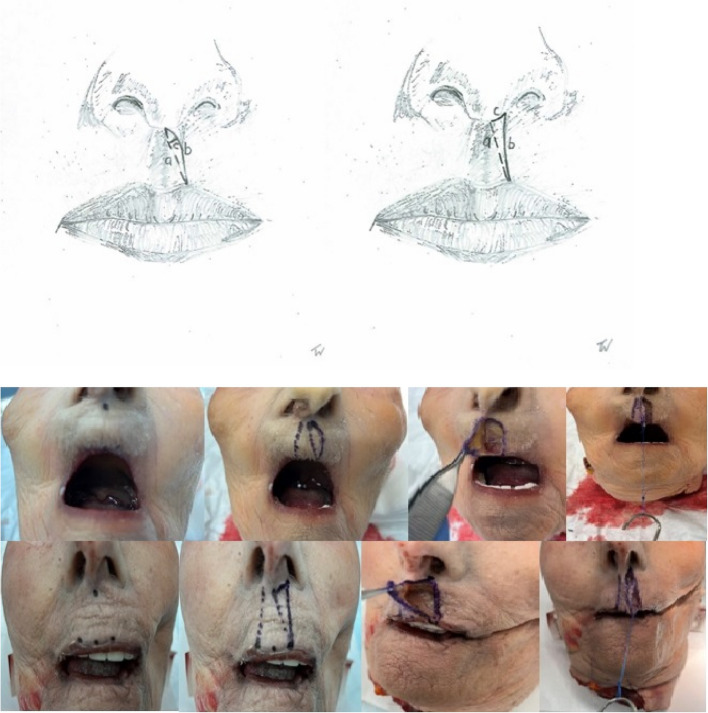
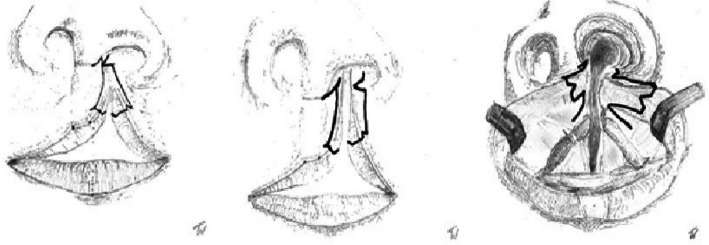
Methods: A study-using 10 adult cadavers-compared two vertical incision lines: the Millard advancement-rotation flap and our Z-back-cut cheiloplasty which reassembles a Z-plasty at the nostril by combining with a back cut at the lower columella rim. A skin distraction model assessed the impact of tension on lengthening. Our technique demonstrated increased vertical height compared to Millard's method. Based on these findings, we applied our approach in clinical settings.
Results: The Millard flap showed significantly less elongation (up to 35%) between the lateral cupid's bow and the columella base than our method. This suggests that the Z-plasty principle is beneficial in unilateral cleft lip closure. Clinical outcomes confirmed its applicability in both partial and complete clefts.
Discussion: Applying our findings in pediatric patients yielded at least equivalent results to the Millard II technique, even in cases with postoperative wound infections and increased contraction risk.
Conclusion: Our research supports integrating Z-plasty principles into unilateral cleft lip repair. We plan to use this technique in future surgeries where indicated.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


