Anna Litwin, Thu Giang Le Thi, Nabil El-Lababidi, Angelika Kindermann, Rouzha Pancheva, Konstantinos Gerasimidis, Cristina Campos Goncalves, Paula Crespo Escobar, Tena Niseteo, Katharina Ikrath, Sibylle Koletzko
{"title":"Celiac disease diagnosis in clinical practice: ESPGHAN quality of care survey from 129 pediatric hospitals across 28 countries.","authors":"Anna Litwin, Thu Giang Le Thi, Nabil El-Lababidi, Angelika Kindermann, Rouzha Pancheva, Konstantinos Gerasimidis, Cristina Campos Goncalves, Paula Crespo Escobar, Tena Niseteo, Katharina Ikrath, Sibylle Koletzko","doi":"10.1002/jpn3.70143","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) guidelines recommend first-line serology for suspected celiac disease (CeD), measuring only transglutaminase antibodies (TGA-immunoglobulin A [IgA]) plus total IgA. If TGA-IgA is ≥10 times the normal value, pediatric gastroenterologists (pedGI) may diagnose CeD without biopsies if autoantibodies against endomysial antibodies (EMA-IgA) are positive in a 2nd blood sample. This Quality-of-Care (QoC) project benchmarked diagnostic workup in clinical practice using ESPGHAN CeD guidelines as reference.</p><p><strong>Methods: </strong>A pseudonymized survey on CeD practices was sent to 141 hospitals within the ESPGHAN QoC-network in 28 countries.</p><p><strong>Results: </strong>Questionnaires were completed by 129/141 (91.5%) hospitals, with 121 (94%) having pedGI staff. As reasons conflicting with good QoC for CeD in their setting, responders assumed knowledge deficits among the public (57%), primary care providers (64%), non-GI physicians (16%), and pedGIs (0%). For initial testing, 66% of physicians ordered only total IgA and TGA-IgA, 7% did not use this combination, and 29% ordered additional serology (TGA-IgG, EMA, antibodies against deaminated gliadin peptide, or native gliadin). Regarding conflicting results for TGA-IgA and histopathology in IgA-sufficient children, 61% incorrectly classified negative TGA-IgA with Marsh 2 and 57% with Marsh 3 lesions as \"potential CeD,\" while 49% excluded CeD in the case of villous atrophy and negative TGA-IgA. Routine practice did not align with the ESPGHAN recommendations regarding performance of duodenal biopsies (27%), EMA-testing (34%), and diagnosis of CeD in IgA-deficient children (32%).</p><p><strong>Conclusions: </strong>We identified areas for improving QoC regarding both effectiveness and efficacy, in pediatric patients with suspected CeD, and consequently developed easy-to-use tools to improve guideline implementation.</p>","PeriodicalId":16694,"journal":{"name":"Journal of Pediatric Gastroenterology and Nutrition","volume":" ","pages":"606-617"},"PeriodicalIF":2.6000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12408967/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Pediatric Gastroenterology and Nutrition","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/jpn3.70143","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/7 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) guidelines recommend first-line serology for suspected celiac disease (CeD), measuring only transglutaminase antibodies (TGA-immunoglobulin A [IgA]) plus total IgA. If TGA-IgA is ≥10 times the normal value, pediatric gastroenterologists (pedGI) may diagnose CeD without biopsies if autoantibodies against endomysial antibodies (EMA-IgA) are positive in a 2nd blood sample. This Quality-of-Care (QoC) project benchmarked diagnostic workup in clinical practice using ESPGHAN CeD guidelines as reference.
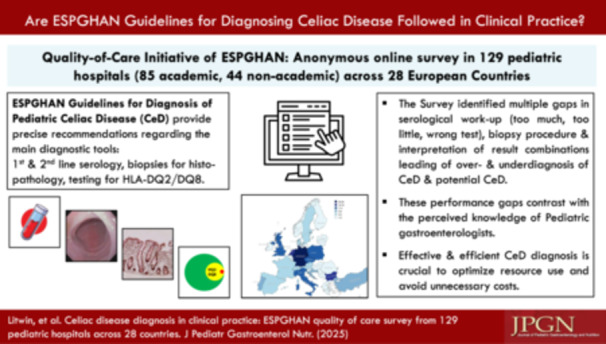
Methods: A pseudonymized survey on CeD practices was sent to 141 hospitals within the ESPGHAN QoC-network in 28 countries.
Results: Questionnaires were completed by 129/141 (91.5%) hospitals, with 121 (94%) having pedGI staff. As reasons conflicting with good QoC for CeD in their setting, responders assumed knowledge deficits among the public (57%), primary care providers (64%), non-GI physicians (16%), and pedGIs (0%). For initial testing, 66% of physicians ordered only total IgA and TGA-IgA, 7% did not use this combination, and 29% ordered additional serology (TGA-IgG, EMA, antibodies against deaminated gliadin peptide, or native gliadin). Regarding conflicting results for TGA-IgA and histopathology in IgA-sufficient children, 61% incorrectly classified negative TGA-IgA with Marsh 2 and 57% with Marsh 3 lesions as "potential CeD," while 49% excluded CeD in the case of villous atrophy and negative TGA-IgA. Routine practice did not align with the ESPGHAN recommendations regarding performance of duodenal biopsies (27%), EMA-testing (34%), and diagnosis of CeD in IgA-deficient children (32%).
Conclusions: We identified areas for improving QoC regarding both effectiveness and efficacy, in pediatric patients with suspected CeD, and consequently developed easy-to-use tools to improve guideline implementation.
期刊介绍:
The Journal of Pediatric Gastroenterology and Nutrition (JPGN) provides a forum for original papers and reviews dealing with pediatric gastroenterology and nutrition, including normal and abnormal functions of the alimentary tract and its associated organs, including the salivary glands, pancreas, gallbladder, and liver. Particular emphasis is on development and its relation to infant and childhood nutrition.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


