{"title":"Meta-analysis of TB & HIV co-infection mortality rate in sub-Saharan African children, youth, and adolescents.","authors":"Fassikaw Kebede Bizuneh, Tsehay Kebede Bizuneh, Getaye Tizazu Biwota, Biruk Beletew Abate, Tilahun Gizaw Ayenew","doi":"10.1186/s13052-025-02019-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Despite the effectiveness of antiretroviral treatment (ART) in reducing morbidity and mortality, children and adolescents with co-infections face an elevated risk of death due to their young age and compromised immune systems. While risk factors for tuberculosis (TB) and adverse TB outcomes in HIV-infected adults are well-documented for mortality estimation, understanding mortality risks among HIV-infected children and adolescents, especially in the era of test and treatment and universal ART for all HIV-infected persons, remains limited. This study aimed to estimate the mortality rate among TB and HIV-co-infected children in Sub-Saharan African countries using SRM.</p><p><strong>Methods: </strong>We systematically searched relevant studies from seven international electronic databases. Articles were searched using Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Article searching included six electronic databases including PubMed/MEDLINE (N = 1287), Scopus (N = 447), Web of Science (N = 174), Science Direct (N = 749, Cochran (N = 57), and Google Scholar and research repository bases searching (N = 42). The quality of primary studies was evaluated using Joanna Briggs Institute (JBI) checklist. The pooled mortality rate was estimated using a weighted inverse variance random-effect meta-analysis. Heterogeneity among studies was assessed using Cochran's Q test and estimated using I2 statistic. This document is registered in Prospero (CRD420251012913).</p><p><strong>Result: </strong>In this SRM, 16 individual studies were included. During the co-infected mortality screening of 5,098 participants, 657 deaths were reported after co-treatment started. The pooled mortality burden was estimated at 12.96% (95% CI: 8.94 to 16.98, I2 = 92.6%, P = 0.001). The majority of TB co-infected cases were newly diagnosed after ART started. The final weighted inverse variance random-effect regression indicated WHO stages III and IV (pooled HR = 4.34), poor/ fair ART adherence (pooled HR = 3.11), missed Isoniazid preventive therapy (IPT) (pooled HR = 3.07), hemoglobin levels ≤ 10 mg/dL (pooled HR = 2.84), bedridden functional status (pooled HR = 3.19), below threshold CD4 count (pooled HR = 1.80), and missed cotrimoxazole preventive therapy (CPT) (pooled AOR = 1.58) were predictors of premature death during co-infection.</p><p><strong>Conclusion: </strong>In this review, the overall pooled burden of mortality in HIV-infected children in SSA countries was high compared with the End TB Strategy target estimation. Significant predictors of mortality included WHO clinical stages III and IV, poor or fair ART adherence, missed Isoniazid preventive therapy (IPT), and hemoglobin levels ≤ 10 mg/dL. Therefore, counseling on antiretroviral therapy adherence should be strengthened; early screening and treating of anemia, screening and scaling up of IPT, critical ART drug, and nutritional counseling should be done during regular visits for caregivers to prevent premature deaths among children, youths, and adolescents during co-infection in SSA.</p>","PeriodicalId":14511,"journal":{"name":"Italian Journal of Pediatrics","volume":"51 1","pages":"210"},"PeriodicalIF":3.1000,"publicationDate":"2025-07-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12232751/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Italian Journal of Pediatrics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13052-025-02019-2","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Despite the effectiveness of antiretroviral treatment (ART) in reducing morbidity and mortality, children and adolescents with co-infections face an elevated risk of death due to their young age and compromised immune systems. While risk factors for tuberculosis (TB) and adverse TB outcomes in HIV-infected adults are well-documented for mortality estimation, understanding mortality risks among HIV-infected children and adolescents, especially in the era of test and treatment and universal ART for all HIV-infected persons, remains limited. This study aimed to estimate the mortality rate among TB and HIV-co-infected children in Sub-Saharan African countries using SRM.
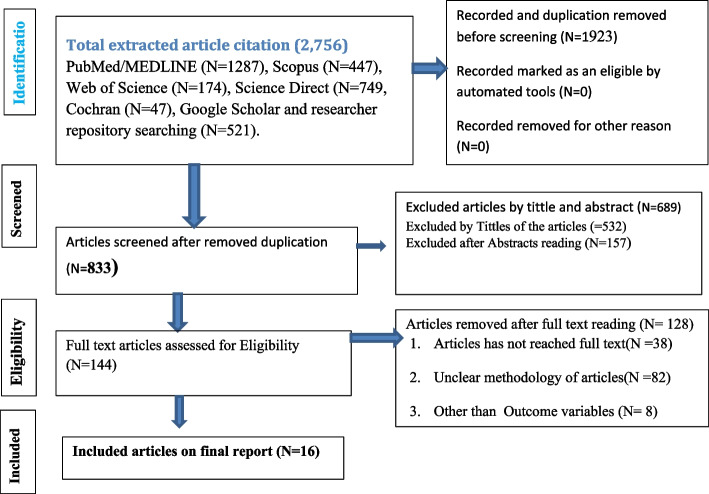
Methods: We systematically searched relevant studies from seven international electronic databases. Articles were searched using Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Article searching included six electronic databases including PubMed/MEDLINE (N = 1287), Scopus (N = 447), Web of Science (N = 174), Science Direct (N = 749, Cochran (N = 57), and Google Scholar and research repository bases searching (N = 42). The quality of primary studies was evaluated using Joanna Briggs Institute (JBI) checklist. The pooled mortality rate was estimated using a weighted inverse variance random-effect meta-analysis. Heterogeneity among studies was assessed using Cochran's Q test and estimated using I2 statistic. This document is registered in Prospero (CRD420251012913).
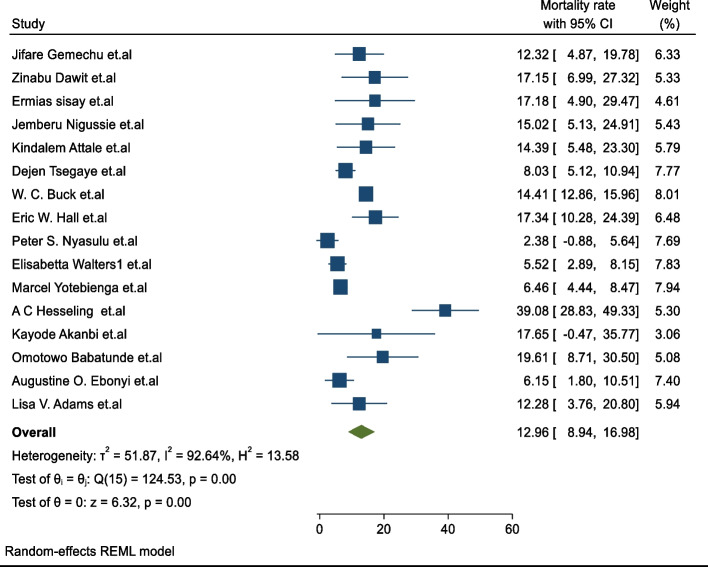
Result: In this SRM, 16 individual studies were included. During the co-infected mortality screening of 5,098 participants, 657 deaths were reported after co-treatment started. The pooled mortality burden was estimated at 12.96% (95% CI: 8.94 to 16.98, I2 = 92.6%, P = 0.001). The majority of TB co-infected cases were newly diagnosed after ART started. The final weighted inverse variance random-effect regression indicated WHO stages III and IV (pooled HR = 4.34), poor/ fair ART adherence (pooled HR = 3.11), missed Isoniazid preventive therapy (IPT) (pooled HR = 3.07), hemoglobin levels ≤ 10 mg/dL (pooled HR = 2.84), bedridden functional status (pooled HR = 3.19), below threshold CD4 count (pooled HR = 1.80), and missed cotrimoxazole preventive therapy (CPT) (pooled AOR = 1.58) were predictors of premature death during co-infection.
Conclusion: In this review, the overall pooled burden of mortality in HIV-infected children in SSA countries was high compared with the End TB Strategy target estimation. Significant predictors of mortality included WHO clinical stages III and IV, poor or fair ART adherence, missed Isoniazid preventive therapy (IPT), and hemoglobin levels ≤ 10 mg/dL. Therefore, counseling on antiretroviral therapy adherence should be strengthened; early screening and treating of anemia, screening and scaling up of IPT, critical ART drug, and nutritional counseling should be done during regular visits for caregivers to prevent premature deaths among children, youths, and adolescents during co-infection in SSA.
期刊介绍:
Italian Journal of Pediatrics is an open access peer-reviewed journal that includes all aspects of pediatric medicine. The journal also covers health service and public health research that addresses primary care issues.
The journal provides a high-quality forum for pediatricians and other healthcare professionals to report and discuss up-to-the-minute research and expert reviews in the field of pediatric medicine. The journal will continue to develop the range of articles published to enable this invaluable resource to stay at the forefront of the field.
Italian Journal of Pediatrics, which commenced in 1975 as Rivista Italiana di Pediatria, provides a high-quality forum for pediatricians and other healthcare professionals to report and discuss up-to-the-minute research and expert reviews in the field of pediatric medicine. The journal will continue to develop the range of articles published to enable this invaluable resource to stay at the forefront of the field.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


