{"title":"Red blood cell transfusion practices in extracorporeal membrane oxygenation: A single-center study.","authors":"Shailesh Balasubramanian, Mahmoud Alwakeel, Divyajot Sadana, Mani Latifi, Chase Donaldson, Brett Wakefield, Edward Soltesz, Kenneth McCurry, Sudhir Krishnan","doi":"10.1111/tme.13154","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Evaluating blood transfusion practices and their impact on morbidity and mortality across extracorporeal membrane oxygenation (ECMO) configurations.</p><p><strong>Background: </strong>As ECMO becomes increasingly utilised in critical care, the ideal Hgb level remains uncertain. While guidelines recommend higher levels, emerging evidence suggests potential harm. Our study addresses this gap by investigating the optimal Hgb level for ECMO.</p><p><strong>Methods: </strong>A retrospective cohort study included all adult patients receiving ECMO between January 2016 and December 2018. The primary outcome assessed the optimal Hgb level associated with reduced ECMO duration and in-hospital mortality. Multivariable and Cox-proportional regression analyses were performed.</p><p><strong>Results: </strong>A total of 306 patients underwent ECMO, with 31 patients having mean Hgb levels 7-7.9 g/dL, 176 patients 8-8.9 g/dL, 72 patients 9-9.9 g/dL, and 27 patients ≥10 g/dL. The mean (SD) age was 56 years (15), with 60.8% male (186/306). ECMO configurations were primarily Venoarterial (VA) (59.8%), followed by Venovenous (VV) (36.9%) and Hybrid (3.3%). The 7-7.9 g/dL Hgb group was associated with longer ECMO duration (mean 17.5 days, coefficient 2.2, 95% CI 0.02-4.4, p = 0.048) compared to the ≥10 g/dL group, with no significant mortality differences across Hgb levels. VA ECMO patients had a significantly higher mortality risk than VV ECMO patients (aHR 2.33, 95% CI 1.50-3.60, p < 0.001). Blood product use, including RBC and Cryo, was associated with longer ECMO duration, while FFP reduced both duration (coefficient - 0.84, 95% CI -1.11--0.57, p < 0.001) and mortality risk (aHR 0.895, 95% CI 0.818-0.973, p = 0.012).</p><p><strong>Conclusion: </strong>Targeting Hgb level >8 g/dL in ECMO patients may help reduce ECMO duration.</p>","PeriodicalId":23306,"journal":{"name":"Transfusion Medicine","volume":" ","pages":"337-345"},"PeriodicalIF":1.4000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12361832/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transfusion Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/tme.13154","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/4 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Evaluating blood transfusion practices and their impact on morbidity and mortality across extracorporeal membrane oxygenation (ECMO) configurations.
Background: As ECMO becomes increasingly utilised in critical care, the ideal Hgb level remains uncertain. While guidelines recommend higher levels, emerging evidence suggests potential harm. Our study addresses this gap by investigating the optimal Hgb level for ECMO.
Methods: A retrospective cohort study included all adult patients receiving ECMO between January 2016 and December 2018. The primary outcome assessed the optimal Hgb level associated with reduced ECMO duration and in-hospital mortality. Multivariable and Cox-proportional regression analyses were performed.
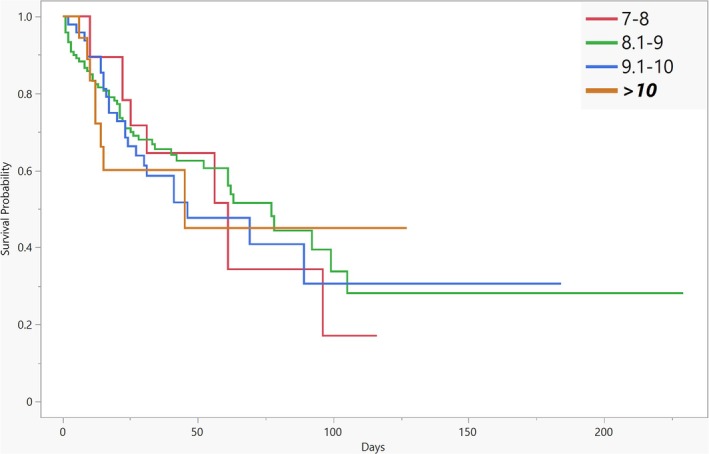
Results: A total of 306 patients underwent ECMO, with 31 patients having mean Hgb levels 7-7.9 g/dL, 176 patients 8-8.9 g/dL, 72 patients 9-9.9 g/dL, and 27 patients ≥10 g/dL. The mean (SD) age was 56 years (15), with 60.8% male (186/306). ECMO configurations were primarily Venoarterial (VA) (59.8%), followed by Venovenous (VV) (36.9%) and Hybrid (3.3%). The 7-7.9 g/dL Hgb group was associated with longer ECMO duration (mean 17.5 days, coefficient 2.2, 95% CI 0.02-4.4, p = 0.048) compared to the ≥10 g/dL group, with no significant mortality differences across Hgb levels. VA ECMO patients had a significantly higher mortality risk than VV ECMO patients (aHR 2.33, 95% CI 1.50-3.60, p < 0.001). Blood product use, including RBC and Cryo, was associated with longer ECMO duration, while FFP reduced both duration (coefficient - 0.84, 95% CI -1.11--0.57, p < 0.001) and mortality risk (aHR 0.895, 95% CI 0.818-0.973, p = 0.012).
Conclusion: Targeting Hgb level >8 g/dL in ECMO patients may help reduce ECMO duration.
期刊介绍:
Transfusion Medicine publishes articles on transfusion medicine in its widest context, including blood transfusion practice (blood procurement, pharmaceutical, clinical, scientific, computing and documentary aspects), immunohaematology, immunogenetics, histocompatibility, medico-legal applications, and related molecular biology and biotechnology.
In addition to original articles, which may include brief communications and case reports, the journal contains a regular educational section (based on invited reviews and state-of-the-art reports), technical section (including quality assurance and current practice guidelines), leading articles, letters to the editor, occasional historical articles and signed book reviews. Some lectures from Society meetings that are likely to be of general interest to readers of the Journal may be published at the discretion of the Editor and subject to the availability of space in the Journal.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


