Susan Dent, Heather Moore, Michael Fradley, Chloe Grace Rose, Stella Stergiopoulos, Connie Chen, Benjamin Li, Avirup Guha
{"title":"QT STAR: concomitant QTc-prolonging medication use among patients with HR+/HER2- metastatic breast cancer receiving a CDK4/6 inhibitor in first line.","authors":"Susan Dent, Heather Moore, Michael Fradley, Chloe Grace Rose, Stella Stergiopoulos, Connie Chen, Benjamin Li, Avirup Guha","doi":"10.1186/s40959-025-00364-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The risk of drug-induced corrected QT interval (QTc) prolongation is an important consideration in clinical decision-making for patients with hormone receptor-positive/human epidermal growth factor receptor 2-negative (HR+/HER2-) metastatic breast cancer (mBC). This retrospective analysis described concomitant QTc-prolonging medication use in patients with HR+/HER2- mBC who received first-line (1L) treatment with a cyclin-dependent kinase 4/6 inhibitor (CDK4/6i) plus an aromatase inhibitor (AI).</p><p><strong>Methods: </strong>This retrospective claims analysis utilized the Optum Clinformatics Data Mart database to identify patients with HR+/HER2- mBC who initiated 1L CDK4/6i plus AI treatment between January 2017 and March 2022. Exposure to QTc-prolonging medications (overall and by Torsades de Pointes [TdP] risk, per www.crediblemeds.org ) was assessed at index (i.e., CDK4/6i treatment initiation) and during follow-up (i.e., duration of CDK4/6i treatment) in the overall cohort and cohorts stratified by patient age.</p><p><strong>Results: </strong>A total of 1517 patients met the study criteria; 33.8%, 35.5%, and 30.8% were aged < 65, 65-74, and ≥ 75 years, respectively. Exposure to ≥ 1 QTc-prolonging medication or ≥ 1 medication with known TdP risk was observed in 53.3% and 15.4% of patients at index, respectively, and 78.6% and 57.1% of patients during follow-up, respectively. Patients were exposed to QTc-prolonging medications for 54.6% of total person-time during follow-up. Patients aged ≥ 65 years had higher exposure to medications with conditional TdP risk than those aged < 65 years, primarily driven by increased diuretic use.</p><p><strong>Conclusions: </strong>QTc-prolonging medication use was common in patients with HR+/HER2- mBC receiving 1L CDK4/6i plus AI treatment, highlighting the importance of reviewing concomitant medications to inform CDK4/6i selection and patient monitoring while on treatment.</p>","PeriodicalId":9804,"journal":{"name":"Cardio-oncology","volume":"11 1","pages":"64"},"PeriodicalIF":3.2000,"publicationDate":"2025-07-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12231290/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardio-oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-025-00364-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The risk of drug-induced corrected QT interval (QTc) prolongation is an important consideration in clinical decision-making for patients with hormone receptor-positive/human epidermal growth factor receptor 2-negative (HR+/HER2-) metastatic breast cancer (mBC). This retrospective analysis described concomitant QTc-prolonging medication use in patients with HR+/HER2- mBC who received first-line (1L) treatment with a cyclin-dependent kinase 4/6 inhibitor (CDK4/6i) plus an aromatase inhibitor (AI).
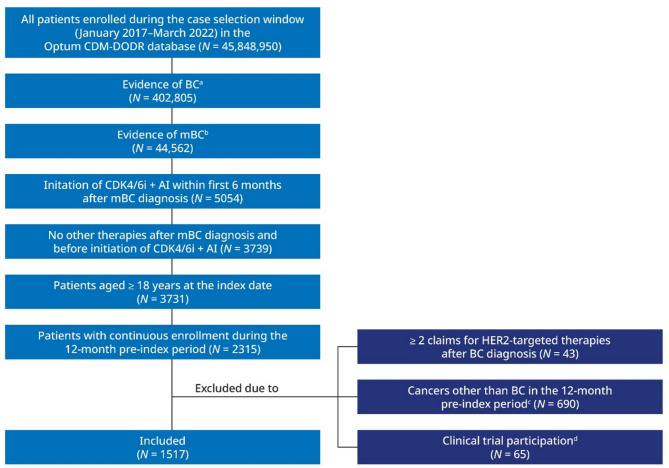
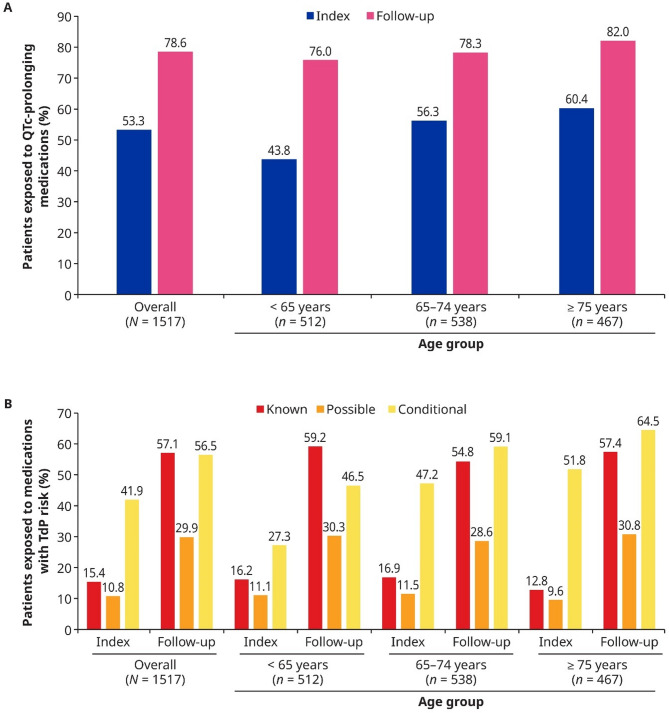
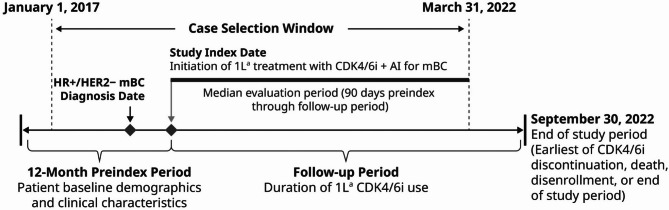
Methods: This retrospective claims analysis utilized the Optum Clinformatics Data Mart database to identify patients with HR+/HER2- mBC who initiated 1L CDK4/6i plus AI treatment between January 2017 and March 2022. Exposure to QTc-prolonging medications (overall and by Torsades de Pointes [TdP] risk, per www.crediblemeds.org ) was assessed at index (i.e., CDK4/6i treatment initiation) and during follow-up (i.e., duration of CDK4/6i treatment) in the overall cohort and cohorts stratified by patient age.
Results: A total of 1517 patients met the study criteria; 33.8%, 35.5%, and 30.8% were aged < 65, 65-74, and ≥ 75 years, respectively. Exposure to ≥ 1 QTc-prolonging medication or ≥ 1 medication with known TdP risk was observed in 53.3% and 15.4% of patients at index, respectively, and 78.6% and 57.1% of patients during follow-up, respectively. Patients were exposed to QTc-prolonging medications for 54.6% of total person-time during follow-up. Patients aged ≥ 65 years had higher exposure to medications with conditional TdP risk than those aged < 65 years, primarily driven by increased diuretic use.
Conclusions: QTc-prolonging medication use was common in patients with HR+/HER2- mBC receiving 1L CDK4/6i plus AI treatment, highlighting the importance of reviewing concomitant medications to inform CDK4/6i selection and patient monitoring while on treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


