The spectrum of overlapping anti-NMDAR encephalitis and demyelinating syndromes: a systematic review of presentation, diagnosis, management, and outcomes.
Saboor Saeed, Huaizhi Wang, Mengjie Jia, Ting Ting Liu, Le Xu, Xuhong Zhang, Shao-Hua Hu
{"title":"The spectrum of overlapping anti-NMDAR encephalitis and demyelinating syndromes: a systematic review of presentation, diagnosis, management, and outcomes.","authors":"Saboor Saeed, Huaizhi Wang, Mengjie Jia, Ting Ting Liu, Le Xu, Xuhong Zhang, Shao-Hua Hu","doi":"10.1080/07853890.2025.2517813","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Anti-NMDAR encephalitis frequently overlaps with demyelinating diseases (MOGAD, NMOSD, MS), creating complex syndromes with diverse presentations and challenging management.</p><p><strong>Methods: </strong>Systematic search of databases including MEDLINE, Google Scholar, Embase, Scopus, Cochrane Library, and Web of Science up to March 2024 for studies on co-existing anti-NMDAR encephalitis and demyelinating syndromes. Data extracted on clinical characteristics, diagnostics, treatments, and outcomes.</p><p><strong>Results: </strong>Twenty-five studies identified 256 patients (16.2%) with co-existing Anti-NMDAR encephalitis and demyelinating syndromes, primarily MOGAD (94.5%), with fewer cases involving NMOSD or MS. The Anti-NMDAR + MOGAD subgroup exhibited seizures (51-72.7%), psychiatric symptoms (45.5-71.4%), cognitive dysfunction (30.6%), and movement disorders (30.6%). All patients had CSF anti-NMDAR antibodies, with MOG (60%) or AQP4 (25%) antibodies. Use of standardized, cell-based assays and adherence to established criteria are essential to avoid false positives, particularly for MOG. MRI abnormalities were seen in 75% of patients. First-line immunotherapies were effective in 70% of cases; 80% of refractory cases responded to second-line therapies.</p><p><strong>Conclusions: </strong>Anti-NMDAR encephalitis overlapping with demyelinating diseases is challenging. Tailored treatments based on detailed immune profiles are key to better outcomes.</p>","PeriodicalId":93874,"journal":{"name":"Annals of medicine","volume":"57 1","pages":"2517813"},"PeriodicalIF":4.3000,"publicationDate":"2025-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12231328/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/07853890.2025.2517813","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/3 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Anti-NMDAR encephalitis frequently overlaps with demyelinating diseases (MOGAD, NMOSD, MS), creating complex syndromes with diverse presentations and challenging management.
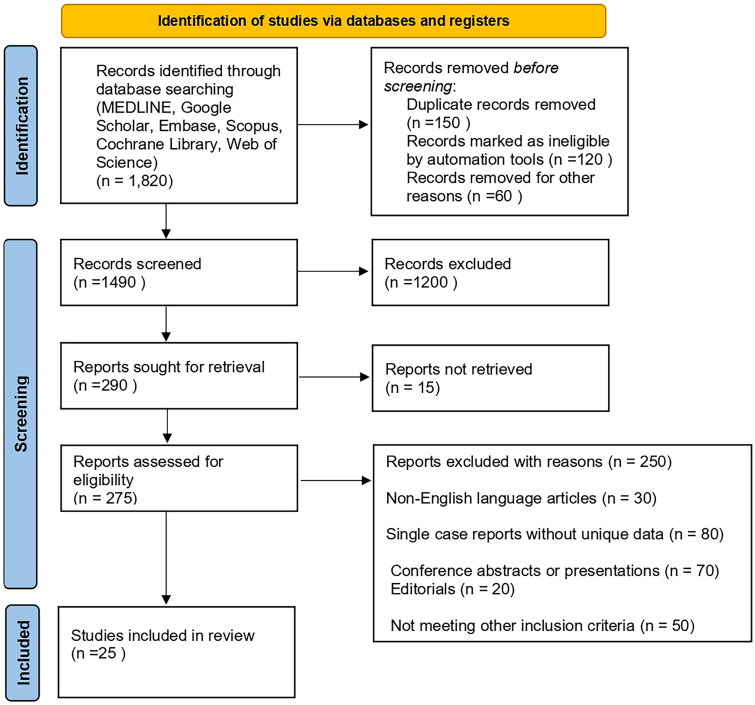
Methods: Systematic search of databases including MEDLINE, Google Scholar, Embase, Scopus, Cochrane Library, and Web of Science up to March 2024 for studies on co-existing anti-NMDAR encephalitis and demyelinating syndromes. Data extracted on clinical characteristics, diagnostics, treatments, and outcomes.
Results: Twenty-five studies identified 256 patients (16.2%) with co-existing Anti-NMDAR encephalitis and demyelinating syndromes, primarily MOGAD (94.5%), with fewer cases involving NMOSD or MS. The Anti-NMDAR + MOGAD subgroup exhibited seizures (51-72.7%), psychiatric symptoms (45.5-71.4%), cognitive dysfunction (30.6%), and movement disorders (30.6%). All patients had CSF anti-NMDAR antibodies, with MOG (60%) or AQP4 (25%) antibodies. Use of standardized, cell-based assays and adherence to established criteria are essential to avoid false positives, particularly for MOG. MRI abnormalities were seen in 75% of patients. First-line immunotherapies were effective in 70% of cases; 80% of refractory cases responded to second-line therapies.
Conclusions: Anti-NMDAR encephalitis overlapping with demyelinating diseases is challenging. Tailored treatments based on detailed immune profiles are key to better outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


