{"title":"Curative Gastrectomy for Advanced Gastric Cancer in a Patient with Idiopathic Multicentric Castleman Disease: A Rare Case Report.","authors":"Ryohei Kawabata, Yuki Ushimaru, Hisashi Hara, Tomohira Takeoka, Yumiko Yasuhara, Terukazu Yoshihara, Akihiro Kitagawa, Takashi Takeda, Hideo Tomihara, Atsushi Naito, Masahiro Murakami, Shingo Noura, Atsushi Miyamoto","doi":"10.70352/scrj.cr.25-0318","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Idiopathic multicentric Castleman disease (iMCD) is a rare lymphoproliferative disorder characterized by systemic inflammation and chronic immunosuppression. When solid malignancies such as gastric cancer arise in patients with iMCD, perioperative management becomes particularly challenging due to nutritional decline, reactive lymphadenopathy, and elevated surgical risk.</p><p><strong>Case presentation: </strong>A 75-year-old man with a 26-year history of suspected iMCD treated with low-dose corticosteroids presented with epigastric discomfort. Endoscopy revealed a Borrmann type 2 lesion, and biopsy confirmed poorly differentiated adenocarcinoma. CT showed mild lymphadenopathy along the lesser curvature and left gastric artery, as well as systemic involvement. Inguinal node biopsy confirmed polyclonal plasma cell proliferation consistent with iMCD. The patient also met the Asian Working Group for Sarcopenia (AWGS) criteria for severe sarcopenia. A multidisciplinary team initiated preoperative respiratory rehabilitation, nutritional support, and resistance exercise therapy. Curative distal gastrectomy with D2 lymphadenectomy was performed without complications. Histopathology revealed pT2N0M0 (pStage IB) disease. Tocilizumab was started 3 months postoperatively, and the patient remains recurrence-free at 24 months.</p><p><strong>Conclusions: </strong>This case highlights that, even in patients with long-standing iMCD and sarcopenia, carefully staged multimodal perioperative care-including accurate nodal evaluation and individualized systemic therapy-can enable successful curative surgery for advanced gastric cancer.</p>","PeriodicalId":22096,"journal":{"name":"Surgical Case Reports","volume":"11 1","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12226139/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.70352/scrj.cr.25-0318","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Idiopathic multicentric Castleman disease (iMCD) is a rare lymphoproliferative disorder characterized by systemic inflammation and chronic immunosuppression. When solid malignancies such as gastric cancer arise in patients with iMCD, perioperative management becomes particularly challenging due to nutritional decline, reactive lymphadenopathy, and elevated surgical risk.
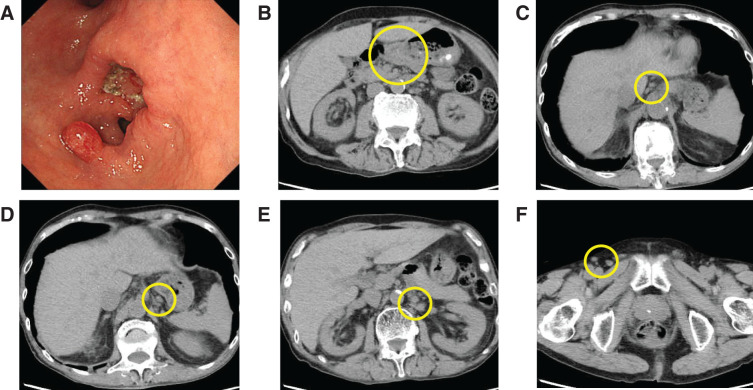
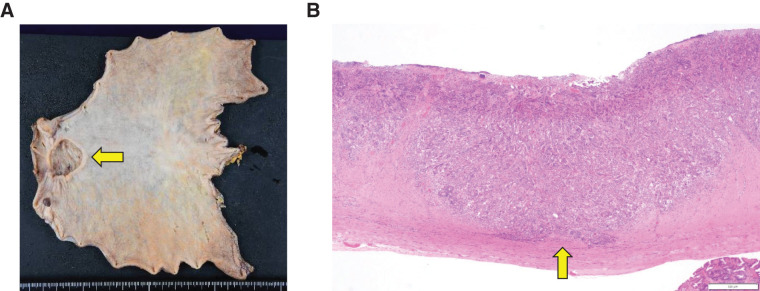
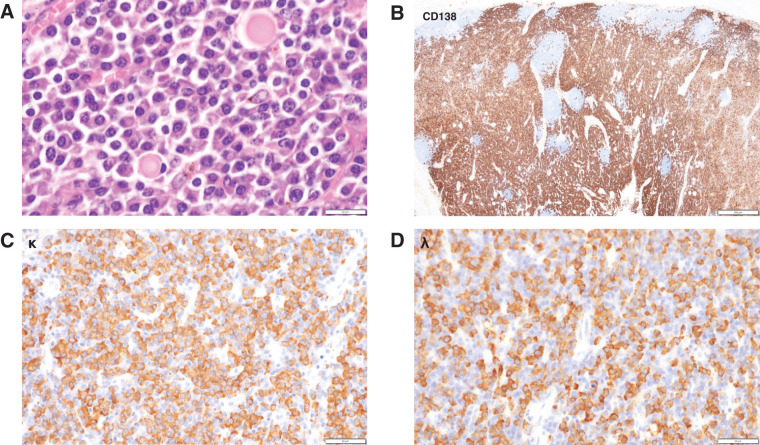
Case presentation: A 75-year-old man with a 26-year history of suspected iMCD treated with low-dose corticosteroids presented with epigastric discomfort. Endoscopy revealed a Borrmann type 2 lesion, and biopsy confirmed poorly differentiated adenocarcinoma. CT showed mild lymphadenopathy along the lesser curvature and left gastric artery, as well as systemic involvement. Inguinal node biopsy confirmed polyclonal plasma cell proliferation consistent with iMCD. The patient also met the Asian Working Group for Sarcopenia (AWGS) criteria for severe sarcopenia. A multidisciplinary team initiated preoperative respiratory rehabilitation, nutritional support, and resistance exercise therapy. Curative distal gastrectomy with D2 lymphadenectomy was performed without complications. Histopathology revealed pT2N0M0 (pStage IB) disease. Tocilizumab was started 3 months postoperatively, and the patient remains recurrence-free at 24 months.
Conclusions: This case highlights that, even in patients with long-standing iMCD and sarcopenia, carefully staged multimodal perioperative care-including accurate nodal evaluation and individualized systemic therapy-can enable successful curative surgery for advanced gastric cancer.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


