Jean Philippe Nesseler, Katrina D Silos, Olivia Peony, Asneh Singh, Patrick Belen, Mitchell R Kamrava, Julie K Jang, Stephen L Shiao, Alan C Kwan, Cody Ramin, Raymond H Mak, Andriana P Nikolova, Katelyn M Atkins
{"title":"Dynamic cardiac changes in low cardiovascular risk patients with triple negative breast cancer treated with chemo-immunotherapy.","authors":"Jean Philippe Nesseler, Katrina D Silos, Olivia Peony, Asneh Singh, Patrick Belen, Mitchell R Kamrava, Julie K Jang, Stephen L Shiao, Alan C Kwan, Cody Ramin, Raymond H Mak, Andriana P Nikolova, Katelyn M Atkins","doi":"10.1186/s40959-025-00361-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Neoadjuvant chemotherapy-immunotherapy is the new standard of care for high-risk early-stage triple negative breast cancer (TNBC). As anthracyclines, pembrolizumab, and radiotherapy may each contribute to an increased risk of cardiovascular events, real-world assessment of early cardiovascular changes is of clinical interest.</p><p><strong>Methods: </strong>Retrospective analysis of 85 women with early-stage TNBC treated with chemotherapy-pembrolizumab between 2018 and 2023 and had ≥ 1 transthoracic echocardiogram (TTE) available. Grade ≥ 2 cardiac common terminology criteria for adverse events (CTCAE) cumulative incidence estimates and Fine-Gray regressions (accounting for non-cardiac death as a competing risk) were calculated. Electrocardiogram (ECG) and TTE parameters during/following systemic therapy (vs. baseline) were compared.</p><p><strong>Results: </strong>The median follow-up from immunotherapy start was 18.7 months [interquartile range (IQR) 13.6-39.1]. The median age was 50 years (IQR 38-61), 19% had hypertension, most (82%) with no detectable coronary artery calcium (CAC = 0), and 0% known cardiovascular disease. 9/85 (11%) experienced a grade ≥2 cardiac event with a median onset of 7.3 months (IQR 4.0-8.0) and a one-year cumulative incidence of 9.6%. Most (7/9) were grade 2 (n = 5 ejection fraction [EF] decline, n = 1 heart failure, n = 1 pericarditis); 2/9 were grade ≥ 3 (myocarditis, urgent percutaneous coronary intervention); all occurred among those receiving carboplatin, paclitaxel, doxorubicin, and cyclophosphamide-based therapy. Adjusting for age and CAC, mean left anterior descending coronary artery radiation dose was associated with an increased risk of cardiac events (sub-distribution hazard ratio 1.16/Gy, 95% confidence interval 1.01-1.35; p = 0.041). QTc prolongation ≥450ms was more common during treatment vs. baseline (39% vs. 15%; p = 0.025). On assessment for recovery, early grade 2 EF decline recovered in 3/5 patients (2/5 with absence of follow-up). In those with baseline and post-treatment TTE, 5/20 (25%) developed new moderate diastolic dysfunction, that persisted in a later TTE in 2/5 patients, downgraded to mild in 1/5, and not reevaluated by TTE in 2/5.</p><p><strong>Conclusion: </strong>Early cardiovascular toxicity was observed during multi-modality TNBC treatment, even in young patients with low cardiovascular risk profiles, highlighting the importance of diligent surveillance. Longer follow-up and further studies are warranted, given the degree of recovery and later effects of these treatments may not yet be fully observed.</p>","PeriodicalId":9804,"journal":{"name":"Cardio-oncology","volume":"11 1","pages":"62"},"PeriodicalIF":3.2000,"publicationDate":"2025-07-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12225161/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardio-oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-025-00361-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Neoadjuvant chemotherapy-immunotherapy is the new standard of care for high-risk early-stage triple negative breast cancer (TNBC). As anthracyclines, pembrolizumab, and radiotherapy may each contribute to an increased risk of cardiovascular events, real-world assessment of early cardiovascular changes is of clinical interest.
Methods: Retrospective analysis of 85 women with early-stage TNBC treated with chemotherapy-pembrolizumab between 2018 and 2023 and had ≥ 1 transthoracic echocardiogram (TTE) available. Grade ≥ 2 cardiac common terminology criteria for adverse events (CTCAE) cumulative incidence estimates and Fine-Gray regressions (accounting for non-cardiac death as a competing risk) were calculated. Electrocardiogram (ECG) and TTE parameters during/following systemic therapy (vs. baseline) were compared.
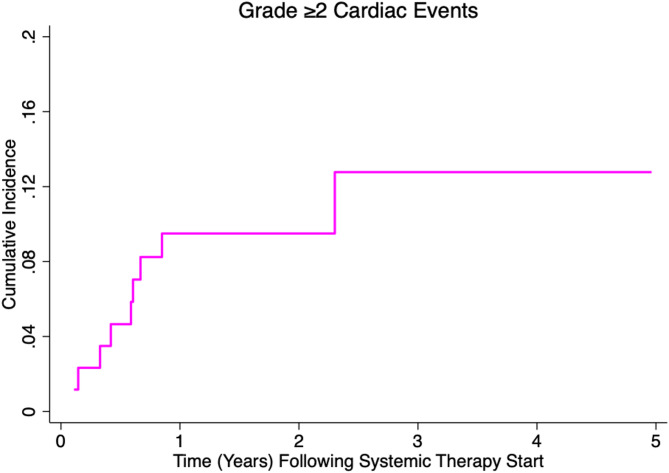
Results: The median follow-up from immunotherapy start was 18.7 months [interquartile range (IQR) 13.6-39.1]. The median age was 50 years (IQR 38-61), 19% had hypertension, most (82%) with no detectable coronary artery calcium (CAC = 0), and 0% known cardiovascular disease. 9/85 (11%) experienced a grade ≥2 cardiac event with a median onset of 7.3 months (IQR 4.0-8.0) and a one-year cumulative incidence of 9.6%. Most (7/9) were grade 2 (n = 5 ejection fraction [EF] decline, n = 1 heart failure, n = 1 pericarditis); 2/9 were grade ≥ 3 (myocarditis, urgent percutaneous coronary intervention); all occurred among those receiving carboplatin, paclitaxel, doxorubicin, and cyclophosphamide-based therapy. Adjusting for age and CAC, mean left anterior descending coronary artery radiation dose was associated with an increased risk of cardiac events (sub-distribution hazard ratio 1.16/Gy, 95% confidence interval 1.01-1.35; p = 0.041). QTc prolongation ≥450ms was more common during treatment vs. baseline (39% vs. 15%; p = 0.025). On assessment for recovery, early grade 2 EF decline recovered in 3/5 patients (2/5 with absence of follow-up). In those with baseline and post-treatment TTE, 5/20 (25%) developed new moderate diastolic dysfunction, that persisted in a later TTE in 2/5 patients, downgraded to mild in 1/5, and not reevaluated by TTE in 2/5.
Conclusion: Early cardiovascular toxicity was observed during multi-modality TNBC treatment, even in young patients with low cardiovascular risk profiles, highlighting the importance of diligent surveillance. Longer follow-up and further studies are warranted, given the degree of recovery and later effects of these treatments may not yet be fully observed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


