Alice Terrett, Athena Chin, Mihye Kwon, Samuel Whittle, Catherine Hill
{"title":"Perioperative management with DMARDs in rheumatic diseases: a scoping review of clinical guidelines.","authors":"Alice Terrett, Athena Chin, Mihye Kwon, Samuel Whittle, Catherine Hill","doi":"10.1186/s41927-025-00522-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Patients with autoimmune rheumatic diseases have high rates of surgical procedures including joint replacements despite the use of disease-modifying anti-rheumatic drugs (DMARDs). This scoping review compares clinical practice guideline recommendations for the perioperative management of DMARDs in such patients.</p><p><strong>Methods: </strong>Medline and EMBASE were searched, and a hand search of references was performed to obtain guidelines published since 2014 by national/international academic societies in rheumatology addressing perioperative management of DMARDs in any of adult rheumatoid arthritis (RA), ankylosing spondylitis (AS), psoriatic arthritis (PsA), juvenile idiopathic arthritis (JIA) or systemic lupus erythematosus (SLE). Data extraction was performed in duplicate by two authors.</p><p><strong>Results: </strong>Twelve guidelines were included - 10 (83%) incorporated a perioperative recommendation within a broader guideline. RA was the sole rheumatic condition in 6 (50%) guidelines. Low-moderate quality evidence supported these recommendations, based on evidence from studies of participants undergoing elective orthopaedic surgery. Guidelines varied in development process, format, the choice of evidence system, level of evidence, strength of recommendation and recommendations for biologic DMARD (bDMARD) use and timing of surgery.</p><p><strong>Conclusion: </strong>Although guidelines for the use of DMARDs in the perioperative period are widely available, the development process and recommendations vary between guidelines. There is a lack of high quality evidence to support recommendations for non-elective, non-orthopaedic surgery cases. Variations in recommendations for bDMARDs in the perioperative period were common, potentially leading to more practice variation in bDMARD use in the perioperative period. Continued accrual and review of evidence will provide greater support for recommendations in this clinical setting.</p>","PeriodicalId":9150,"journal":{"name":"BMC Rheumatology","volume":"9 1","pages":"81"},"PeriodicalIF":2.5000,"publicationDate":"2025-07-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12224603/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41927-025-00522-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Patients with autoimmune rheumatic diseases have high rates of surgical procedures including joint replacements despite the use of disease-modifying anti-rheumatic drugs (DMARDs). This scoping review compares clinical practice guideline recommendations for the perioperative management of DMARDs in such patients.
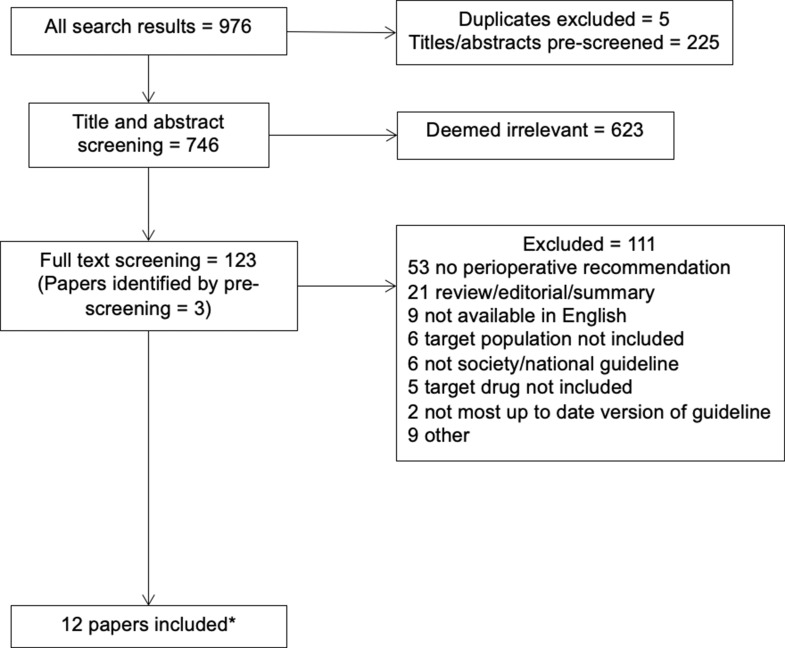
Methods: Medline and EMBASE were searched, and a hand search of references was performed to obtain guidelines published since 2014 by national/international academic societies in rheumatology addressing perioperative management of DMARDs in any of adult rheumatoid arthritis (RA), ankylosing spondylitis (AS), psoriatic arthritis (PsA), juvenile idiopathic arthritis (JIA) or systemic lupus erythematosus (SLE). Data extraction was performed in duplicate by two authors.
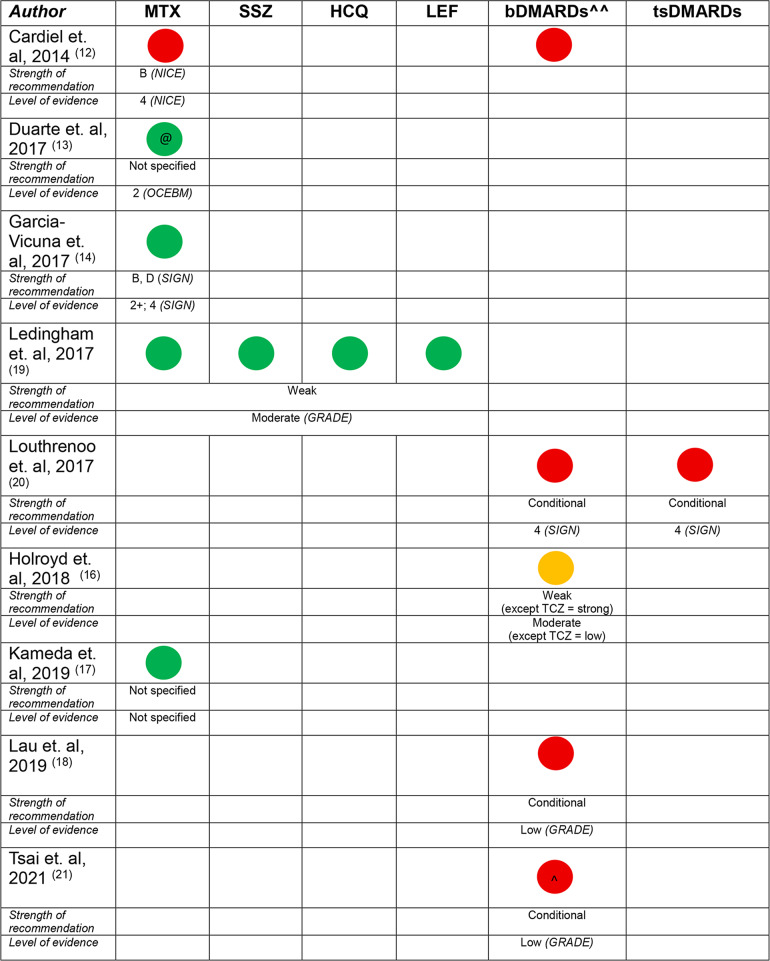
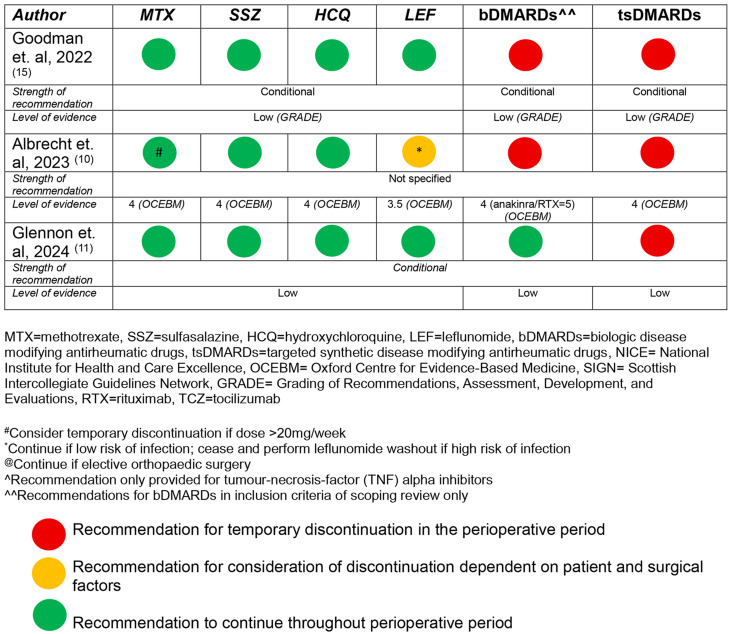
Results: Twelve guidelines were included - 10 (83%) incorporated a perioperative recommendation within a broader guideline. RA was the sole rheumatic condition in 6 (50%) guidelines. Low-moderate quality evidence supported these recommendations, based on evidence from studies of participants undergoing elective orthopaedic surgery. Guidelines varied in development process, format, the choice of evidence system, level of evidence, strength of recommendation and recommendations for biologic DMARD (bDMARD) use and timing of surgery.
Conclusion: Although guidelines for the use of DMARDs in the perioperative period are widely available, the development process and recommendations vary between guidelines. There is a lack of high quality evidence to support recommendations for non-elective, non-orthopaedic surgery cases. Variations in recommendations for bDMARDs in the perioperative period were common, potentially leading to more practice variation in bDMARD use in the perioperative period. Continued accrual and review of evidence will provide greater support for recommendations in this clinical setting.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


