An economic evaluation of a hospital-wide bundle intervention to reduce hospital-acquired infections and bladder distension among hip fracture patients in Sweden.
Sneha Abdul Jabbar, Maria Frödin, Ewa Wikström, Brigid M Gillespie, Hanna Gyllensten, Annette Erichsen
{"title":"An economic evaluation of a hospital-wide bundle intervention to reduce hospital-acquired infections and bladder distension among hip fracture patients in Sweden.","authors":"Sneha Abdul Jabbar, Maria Frödin, Ewa Wikström, Brigid M Gillespie, Hanna Gyllensten, Annette Erichsen","doi":"10.1186/s13756-025-01573-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A theory-driven knowledge translation program was established to co-create and implement evidence-based practices to prevent urinary catheter-associated urinary tract infections (UC-UTIs) and bladder distension (BD). This study investigates the cost-effectiveness of implementing the Safe Hands and Safe Bladder bundle intervention compared to standard care for patients undergoing hip fracture surgery in Sweden.</p><p><strong>Method: </strong>The study included outcomes from a quality register of patients who underwent hip fracture surgery at a Swedish hospital from 2015 to 2020. Adopting a healthcare perspective, estimates for the implementation cost were derived using activity-based costing, while the bundle's cost-effectiveness was estimated using a decision tree model. Health outcomes were evaluated based on adverse events, specifically UC-UTI and BD. Analyses included calculating the incremental cost-effectiveness ratio (ICER), which denotes the incremental cost per added infection rate expressed as a percentage. Additionally, sensitivity analyses were conducted to test the robustness of the results under alternative cost assumptions.</p><p><strong>Results: </strong>The likelihood of avoiding BD or UC-UTI increased from 50 to 87% over the course of the intervention year. The discounted implementation cost was SEK 890,389 (corresponding to Int$ 102,721). However, the implementation cost was offset by costs for a prolonged hospital stay due to these adverse events, resulting in an overall cost savings of SEK - 7,334 per patient (Int$ -846) in 2020 compared to before the intervention was introduced. Consequently, the intervention proved to be cost-effective, leading to savings and a decrease in the occurrence of adverse events.</p><p><strong>Conclusion: </strong>Implementing the bundle intervention in units providing care for patients with acute hip fractures proved cost-effective. This offers decision makers valuable insights and demonstrates that implementation programs incorporating collaboration, facilitation and co-creation processes can effectively use limited resources. Further research should determine the generalizability of the findings to other settings and populations.</p><p><strong>Clinicaltrials: </strong></p><p><strong>Gov registration: </strong>NCT02983136 and ISRCTN 17,022,695, retrospectively registered after data collection were completed.</p>","PeriodicalId":7950,"journal":{"name":"Antimicrobial Resistance and Infection Control","volume":"14 1","pages":"80"},"PeriodicalIF":4.4000,"publicationDate":"2025-07-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12226840/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Antimicrobial Resistance and Infection Control","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13756-025-01573-y","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: A theory-driven knowledge translation program was established to co-create and implement evidence-based practices to prevent urinary catheter-associated urinary tract infections (UC-UTIs) and bladder distension (BD). This study investigates the cost-effectiveness of implementing the Safe Hands and Safe Bladder bundle intervention compared to standard care for patients undergoing hip fracture surgery in Sweden.
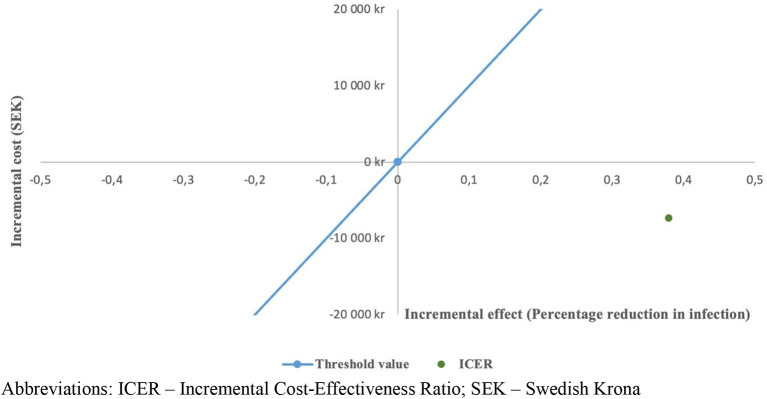
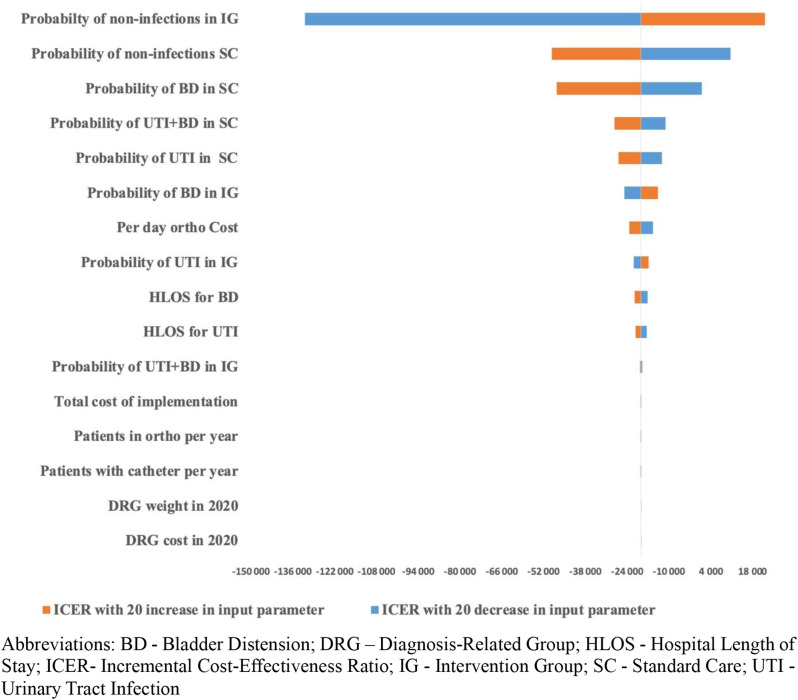
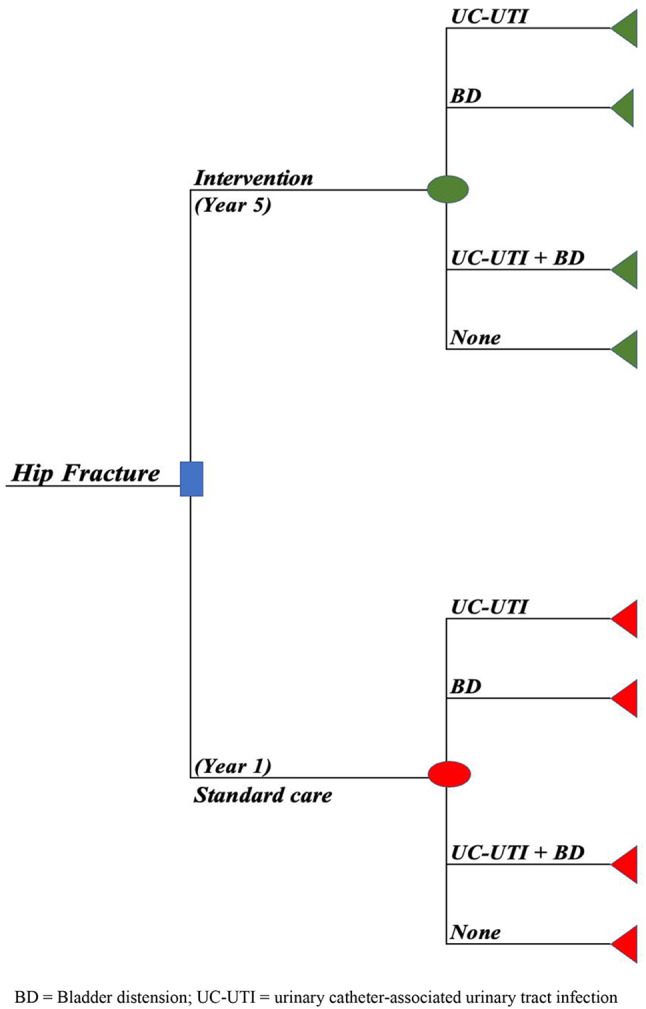
Method: The study included outcomes from a quality register of patients who underwent hip fracture surgery at a Swedish hospital from 2015 to 2020. Adopting a healthcare perspective, estimates for the implementation cost were derived using activity-based costing, while the bundle's cost-effectiveness was estimated using a decision tree model. Health outcomes were evaluated based on adverse events, specifically UC-UTI and BD. Analyses included calculating the incremental cost-effectiveness ratio (ICER), which denotes the incremental cost per added infection rate expressed as a percentage. Additionally, sensitivity analyses were conducted to test the robustness of the results under alternative cost assumptions.
Results: The likelihood of avoiding BD or UC-UTI increased from 50 to 87% over the course of the intervention year. The discounted implementation cost was SEK 890,389 (corresponding to Int$ 102,721). However, the implementation cost was offset by costs for a prolonged hospital stay due to these adverse events, resulting in an overall cost savings of SEK - 7,334 per patient (Int$ -846) in 2020 compared to before the intervention was introduced. Consequently, the intervention proved to be cost-effective, leading to savings and a decrease in the occurrence of adverse events.
Conclusion: Implementing the bundle intervention in units providing care for patients with acute hip fractures proved cost-effective. This offers decision makers valuable insights and demonstrates that implementation programs incorporating collaboration, facilitation and co-creation processes can effectively use limited resources. Further research should determine the generalizability of the findings to other settings and populations.
Clinicaltrials:
Gov registration: NCT02983136 and ISRCTN 17,022,695, retrospectively registered after data collection were completed.
期刊介绍:
Antimicrobial Resistance and Infection Control is a global forum for all those working on the prevention, diagnostic and treatment of health-care associated infections and antimicrobial resistance development in all health-care settings. The journal covers a broad spectrum of preeminent practices and best available data to the top interventional and translational research, and innovative developments in the field of infection control.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


