Longitudinal Innate and Heterologous Adaptive Immune Responses to SARS-CoV-2 JN.1 in Transplant Recipients With Prior Omicron Infection: Limited Neutralization but Robust CD4+ T-Cell Activity.
Victor H Ferreira, Brandon Keith, Faranak Mavandadnejad, Alejandro Ferro, Sara Marocco, Golnaz Amidpour, Alexandra Kurtesi, Freda Qi, Anne-Claude Gingras, Victoria G Hall, Deepali Kumar, Atul Humar
{"title":"Longitudinal Innate and Heterologous Adaptive Immune Responses to SARS-CoV-2 JN.1 in Transplant Recipients With Prior Omicron Infection: Limited Neutralization but Robust CD4<sup>+</sup> T-Cell Activity.","authors":"Victor H Ferreira, Brandon Keith, Faranak Mavandadnejad, Alejandro Ferro, Sara Marocco, Golnaz Amidpour, Alexandra Kurtesi, Freda Qi, Anne-Claude Gingras, Victoria G Hall, Deepali Kumar, Atul Humar","doi":"10.1111/tid.70067","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Solid organ transplant (SOT) recipients are at increased risk for severe COVID-19 and often exhibit reduced vaccine efficacy due to chronic immunosuppression. As new SARS-CoV-2 variants emerge, understanding immune responses following natural infection remains critical for informing protection strategies in this vulnerable population. We conducted a longitudinal study of SOT recipients who had recovered from Omicron BA.1 or BA.2 infection, evaluating immune responses to the JN.1 subvariant at 4-6 weeks and 1 year postinfection.</p><p><strong>Methods: </strong>Neutralizing antibodies to JN.1 were measured using a pseudovirus neutralization assay, and JN.1-specific T-cell responses were assessed by flow cytometry. Frequencies of bulk T-cells and innate immune cells, identified via flow cytometry, and their correlation with adaptive responses were also analyzed.</p><p><strong>Results: </strong>At 4-6 weeks, 30% of participants had detectable JN.1-neutralizing antibodies, rising to 43% at one year, although titers remained low. In contrast, CD4⁺ T-cell responses were robust and detected in 75%-83% of participants at 4-6 weeks, increasing to 75%-93% by 1 year. CD8⁺ T-cell responses were observed less frequently. Exploratory correlations between innate and bulk T-cell subsets with heterologous adaptive immune responses were investigated but did not reveal statistically significant relationships.</p><p><strong>Conclusion: </strong>These findings offer important insights into the durability and breadth of immunity following natural infection in immunocompromised transplant recipients. While heterologous neutralizing antibodies were limited, sustained CD4<sup>+</sup> T-cell responses may help mitigate severe disease following exposure to JN.1-derived variants, which continue to dominate the SARS-CoV-2 landscape.</p>","PeriodicalId":23318,"journal":{"name":"Transplant Infectious Disease","volume":" ","pages":"e70067"},"PeriodicalIF":2.6000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12416463/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplant Infectious Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/tid.70067","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/2 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Solid organ transplant (SOT) recipients are at increased risk for severe COVID-19 and often exhibit reduced vaccine efficacy due to chronic immunosuppression. As new SARS-CoV-2 variants emerge, understanding immune responses following natural infection remains critical for informing protection strategies in this vulnerable population. We conducted a longitudinal study of SOT recipients who had recovered from Omicron BA.1 or BA.2 infection, evaluating immune responses to the JN.1 subvariant at 4-6 weeks and 1 year postinfection.
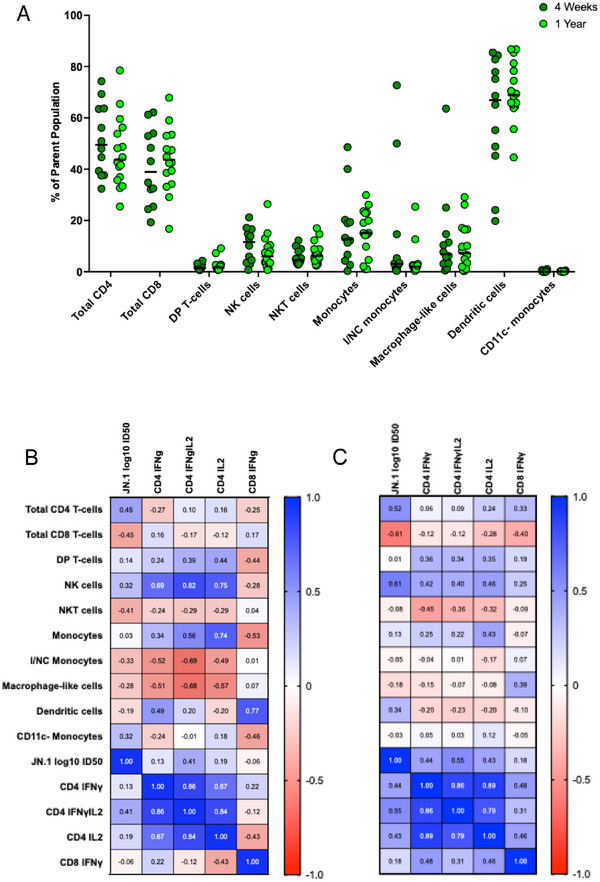
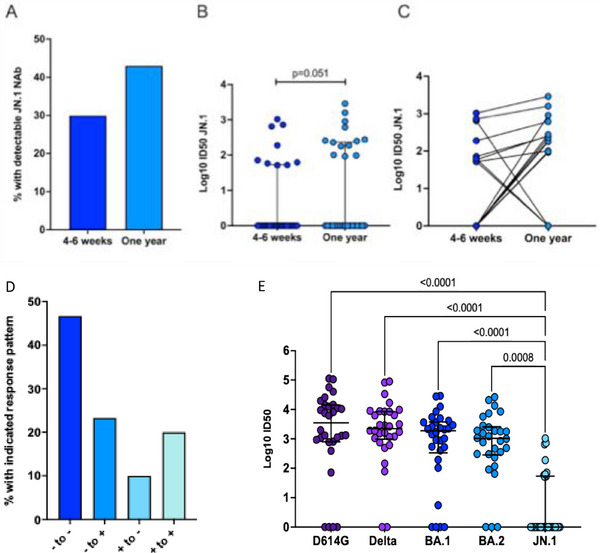
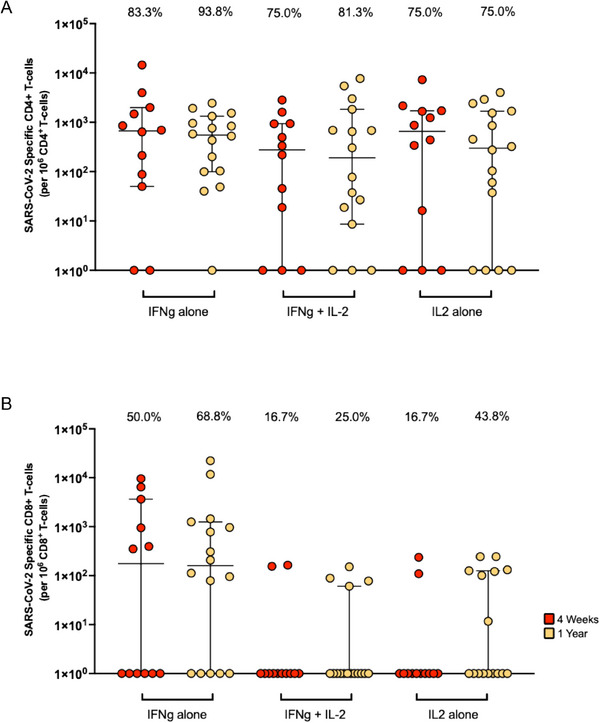
Methods: Neutralizing antibodies to JN.1 were measured using a pseudovirus neutralization assay, and JN.1-specific T-cell responses were assessed by flow cytometry. Frequencies of bulk T-cells and innate immune cells, identified via flow cytometry, and their correlation with adaptive responses were also analyzed.
Results: At 4-6 weeks, 30% of participants had detectable JN.1-neutralizing antibodies, rising to 43% at one year, although titers remained low. In contrast, CD4⁺ T-cell responses were robust and detected in 75%-83% of participants at 4-6 weeks, increasing to 75%-93% by 1 year. CD8⁺ T-cell responses were observed less frequently. Exploratory correlations between innate and bulk T-cell subsets with heterologous adaptive immune responses were investigated but did not reveal statistically significant relationships.
Conclusion: These findings offer important insights into the durability and breadth of immunity following natural infection in immunocompromised transplant recipients. While heterologous neutralizing antibodies were limited, sustained CD4+ T-cell responses may help mitigate severe disease following exposure to JN.1-derived variants, which continue to dominate the SARS-CoV-2 landscape.
期刊介绍:
Transplant Infectious Disease has been established as a forum for presenting the most current information on the prevention and treatment of infection complicating organ and bone marrow transplantation. The point of view of the journal is that infection and allograft rejection (or graft-versus-host disease) are closely intertwined, and that advances in one area will have immediate consequences on the other. The interaction of the transplant recipient with potential microbial invaders, the impact of immunosuppressive strategies on this interaction, and the effects of cytokines, growth factors, and chemokines liberated during the course of infections, rejection, or graft-versus-host disease are central to the interests and mission of this journal.
Transplant Infectious Disease is aimed at disseminating the latest information relevant to the infectious disease complications of transplantation to clinicians and scientists involved in bone marrow, kidney, liver, heart, lung, intestinal, and pancreatic transplantation. The infectious disease consequences and concerns regarding innovative transplant strategies, from novel immunosuppressive agents to xenotransplantation, are very much a concern of this journal. In addition, this journal feels a particular responsibility to inform primary care practitioners in the community, who increasingly are sharing the responsibility for the care of these patients, of the special considerations regarding the prevention and treatment of infection in transplant recipients. As exemplified by the international editorial board, articles are sought throughout the world that address both general issues and those of a more restricted geographic import.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


