Jan Clerinx, Ula Maniewski, Steven Van Den Broucke, Patrick Soentjens, Liselotte Cnops, Marjan Van Esbroeck, Emmanuel Bottieau
{"title":"Acute schistosomiasis in travellers: outcomes of a short-course therapy.","authors":"Jan Clerinx, Ula Maniewski, Steven Van Den Broucke, Patrick Soentjens, Liselotte Cnops, Marjan Van Esbroeck, Emmanuel Bottieau","doi":"10.1093/jtm/taaf065","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Therapy of acute schistosomiasis in travellers currently relies on poorly consistent combinations of corticosteroids and praziquantel. In a cluster of travellers recently infected with Schistosoma mattheei × Schistosoma haematobium hybrids during a trip to South Africa in 2017, we evaluated the safety and efficacy of short methylprednisolone cycles to suppress early symptoms and of a single-day praziquantel/methylprednisolone administration at well-defined time lapses.</p><p><strong>Methods: </strong>Symptomatic patients seen during the early phase, 4 to 5 weeks (week 4-5) after infection, were given oral methylprednisolone 0.5 mg/kg once daily in one or more cycles of three consecutive days until symptoms abated. Patients were seen again at week 7-8 to be given praziquantel 40 mg/kg in two divided doses 2 hours apart, followed by a single dose of oral methylprednisolone 0.5 mg/kg 2 hours later to prevent symptom exacerbation. All patients were reevaluated for symptoms and infection at week 12-14, using serum circulating anodic antigen (CAA) as a marker of active infection.</p><p><strong>Results: </strong>A total of 34 infected individuals were longitudinally followed up. Of these, 21 patients with symptoms at presentation (week 4-5) were given methylprednisolone. Symptoms abated during the first three-day cycle in 15/21 (71%), during the second cycle in another 4/21 (19%), and during the third cycle in the remaining 2/21 (10%). All 34 participants were treated with the praziquantel/steroid combination at week 7-8; 9 (26%) had mild symptoms of short duration. Only 4 (12%) developed fever and needed 1 or 2 additional days of steroids. At week 12-14, serum CAA remained detectable in only one of the 34 participants.</p><p><strong>Conclusion: </strong>In most patients, a single three-day course of methylprednisolone was sufficient to suppress symptoms of acute schistosomiasis. Only few patients experienced short lived symptom exacerbation after taking a single-day praziquantel and methylprednisolone combination at 7-8 weeks following exposure. Infection was cleared in almost all cases 4-6 weeks later.</p>","PeriodicalId":17407,"journal":{"name":"Journal of travel medicine","volume":" ","pages":""},"PeriodicalIF":6.4000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12491658/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of travel medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/jtm/taaf065","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Therapy of acute schistosomiasis in travellers currently relies on poorly consistent combinations of corticosteroids and praziquantel. In a cluster of travellers recently infected with Schistosoma mattheei × Schistosoma haematobium hybrids during a trip to South Africa in 2017, we evaluated the safety and efficacy of short methylprednisolone cycles to suppress early symptoms and of a single-day praziquantel/methylprednisolone administration at well-defined time lapses.
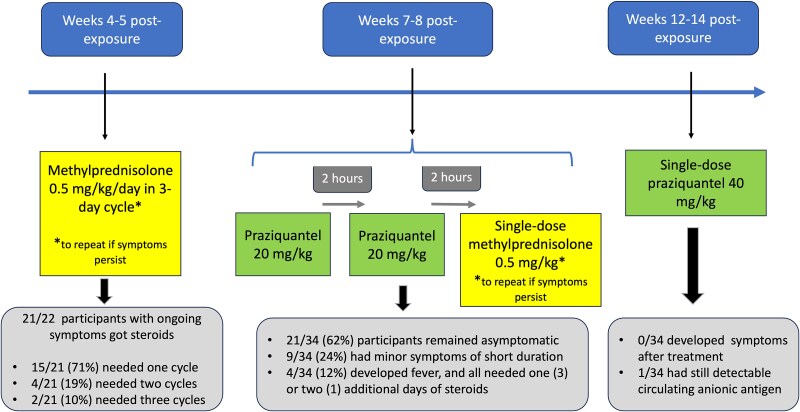
Methods: Symptomatic patients seen during the early phase, 4 to 5 weeks (week 4-5) after infection, were given oral methylprednisolone 0.5 mg/kg once daily in one or more cycles of three consecutive days until symptoms abated. Patients were seen again at week 7-8 to be given praziquantel 40 mg/kg in two divided doses 2 hours apart, followed by a single dose of oral methylprednisolone 0.5 mg/kg 2 hours later to prevent symptom exacerbation. All patients were reevaluated for symptoms and infection at week 12-14, using serum circulating anodic antigen (CAA) as a marker of active infection.
Results: A total of 34 infected individuals were longitudinally followed up. Of these, 21 patients with symptoms at presentation (week 4-5) were given methylprednisolone. Symptoms abated during the first three-day cycle in 15/21 (71%), during the second cycle in another 4/21 (19%), and during the third cycle in the remaining 2/21 (10%). All 34 participants were treated with the praziquantel/steroid combination at week 7-8; 9 (26%) had mild symptoms of short duration. Only 4 (12%) developed fever and needed 1 or 2 additional days of steroids. At week 12-14, serum CAA remained detectable in only one of the 34 participants.
Conclusion: In most patients, a single three-day course of methylprednisolone was sufficient to suppress symptoms of acute schistosomiasis. Only few patients experienced short lived symptom exacerbation after taking a single-day praziquantel and methylprednisolone combination at 7-8 weeks following exposure. Infection was cleared in almost all cases 4-6 weeks later.
期刊介绍:
The Journal of Travel Medicine is a publication that focuses on travel medicine and its intersection with other disciplines. It publishes cutting-edge research, consensus papers, policy papers, and expert reviews. The journal is affiliated with the Asia Pacific Travel Health Society.
The journal's main areas of interest include the prevention and management of travel-associated infections, non-communicable diseases, vaccines, malaria prevention and treatment, multi-drug resistant pathogens, and surveillance on all individuals crossing international borders.
The Journal of Travel Medicine is indexed in multiple major indexing services, including Adis International Ltd., CABI, EBSCOhost, Elsevier BV, Gale, Journal Watch Infectious Diseases (Online), MetaPress, National Library of Medicine, OCLC, Ovid, ProQuest, Thomson Reuters, and the U.S. National Library of Medicine.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


