{"title":"Primary treated versus referred trunk and extremities soft tissue sarcomas: comparative analysis of initial treatment impact on disease control.","authors":"Walter S Nardi, Lucía Aragone, Sergio D Quildrian","doi":"10.3332/ecancer.2025.1933","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Soft tissue sarcomas (STS) are rare and aggressive tumours that require a complex multimodal treatment at referral centers. However, they are often misdiagnosed and subsequently improperly treated at non-specialised centers. A multidisciplinary approach is mandatory for these tumours, involving multiple specialties. Therefore, management should be carried out in reference centers for STS. We aimed to compare oncological outcomes of trunk and extremities STS primarily treated at a reference center versus those referred after initial surgical treatment elsewhere.</p><p><strong>Methods: </strong>All patients with diagnosis of trunk and extremities STS between January 2010 and May 2024, primarily operated at our center or referred after treatment elsewhere, were included. Visceral, retroperitoneal/pelvic, spermatic cord and head/neck STS were excluded, as well as desmoid tumours and dermatofibrosarcoma protuberans subtype. Demographic data and tumour characteristics were evaluated (location, size, French Federation of Cancer Centers Sarcoma Group grade, neo/adjuvant treatment) as well as primary surgery outcomes (R classification). The cohort was divided into two groups: G1 (primary-resection group) and G2 (referred group). Overall survival (OS), local recurrence-local relapse-free survival (LRFS) and distant metastasis-free survival (DMFS) were compared between groups.</p><p><strong>Results: </strong>A total of 102 trunk and extremities STS underwent surgical resection on the mentioned period, out of which 49 were primarily resected (G1) and 53 had previous resections elsewhere (G2: 33 referred for recurrent tumours and 20 referred after inadequate excision). Data on grade was available for 91 lesions and 67% (61/91) were high-grade, with no significant differences between groups. The two groups had statistically significant differences in median tumour size (G1: 9.5 cm versus G2: 4 cm; <i>p</i> < 0.001), preoperative radiotherapy (6 versus 0; <i>p</i> = 0.01) and complete resection margins at first surgery (G1: 46 versus G2 3; <i>p</i> = 0.0001). All patients in G1 had macroscopic complete bloc resections (94% R0 and 6% planned R1 margins). In G2, residual disease was present in 35% (7/20) of the re-resection specimens. All recurrent tumours had macroscopic complete resections at our center (80% R0 and 20% R1 margins). Discussion within a specialised multidisciplinary tumour board was also significantly different between both groups of patients (98% versus 3.8%; <i>p</i> < 0.00001). Three-year LRFS was found to be significantly better when primary surgery was performed at a reference center, with 91% versus 32% (log-rank <i>p</i> < 0.0001). No differences were seen in 3-year DMFS (68.7% versus 72.6%, p = 0.55) and OS (85.3% versus 88.1%, <i>p</i> = 0.72). Positive resection margins at first surgery correlated with worse LRFS (OR 23.1, <i>p</i> = 0.01).</p><p><strong>Conclusion: </strong>Better local control was achieved in patients initially treated at our center. Being surgical margin status is the primary prognostic factor for LRFS, STS should be treated in referral centers where a multidisciplinary approach and proper oncologic resections following sarcomas guidelines recommendations are standard of care. Hence, the importance of a prompt referral even before any intervention in the event of a suspected diagnosis.</p>","PeriodicalId":11460,"journal":{"name":"ecancermedicalscience","volume":"19 ","pages":"1933"},"PeriodicalIF":1.3000,"publicationDate":"2025-06-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12221248/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ecancermedicalscience","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3332/ecancer.2025.1933","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Soft tissue sarcomas (STS) are rare and aggressive tumours that require a complex multimodal treatment at referral centers. However, they are often misdiagnosed and subsequently improperly treated at non-specialised centers. A multidisciplinary approach is mandatory for these tumours, involving multiple specialties. Therefore, management should be carried out in reference centers for STS. We aimed to compare oncological outcomes of trunk and extremities STS primarily treated at a reference center versus those referred after initial surgical treatment elsewhere.
Methods: All patients with diagnosis of trunk and extremities STS between January 2010 and May 2024, primarily operated at our center or referred after treatment elsewhere, were included. Visceral, retroperitoneal/pelvic, spermatic cord and head/neck STS were excluded, as well as desmoid tumours and dermatofibrosarcoma protuberans subtype. Demographic data and tumour characteristics were evaluated (location, size, French Federation of Cancer Centers Sarcoma Group grade, neo/adjuvant treatment) as well as primary surgery outcomes (R classification). The cohort was divided into two groups: G1 (primary-resection group) and G2 (referred group). Overall survival (OS), local recurrence-local relapse-free survival (LRFS) and distant metastasis-free survival (DMFS) were compared between groups.
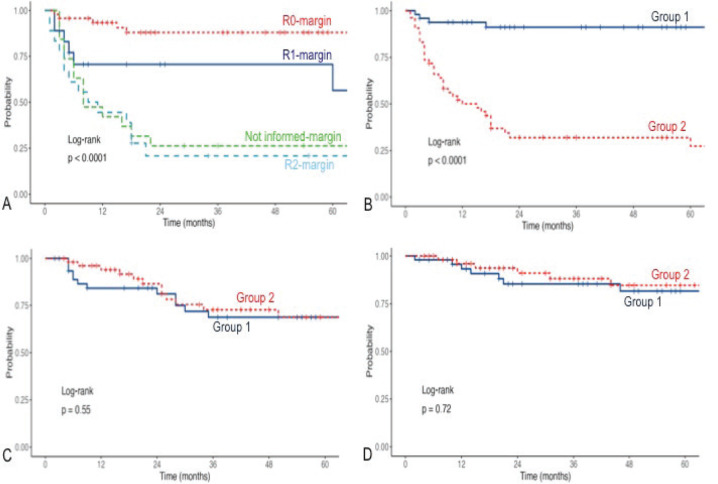
Results: A total of 102 trunk and extremities STS underwent surgical resection on the mentioned period, out of which 49 were primarily resected (G1) and 53 had previous resections elsewhere (G2: 33 referred for recurrent tumours and 20 referred after inadequate excision). Data on grade was available for 91 lesions and 67% (61/91) were high-grade, with no significant differences between groups. The two groups had statistically significant differences in median tumour size (G1: 9.5 cm versus G2: 4 cm; p < 0.001), preoperative radiotherapy (6 versus 0; p = 0.01) and complete resection margins at first surgery (G1: 46 versus G2 3; p = 0.0001). All patients in G1 had macroscopic complete bloc resections (94% R0 and 6% planned R1 margins). In G2, residual disease was present in 35% (7/20) of the re-resection specimens. All recurrent tumours had macroscopic complete resections at our center (80% R0 and 20% R1 margins). Discussion within a specialised multidisciplinary tumour board was also significantly different between both groups of patients (98% versus 3.8%; p < 0.00001). Three-year LRFS was found to be significantly better when primary surgery was performed at a reference center, with 91% versus 32% (log-rank p < 0.0001). No differences were seen in 3-year DMFS (68.7% versus 72.6%, p = 0.55) and OS (85.3% versus 88.1%, p = 0.72). Positive resection margins at first surgery correlated with worse LRFS (OR 23.1, p = 0.01).
Conclusion: Better local control was achieved in patients initially treated at our center. Being surgical margin status is the primary prognostic factor for LRFS, STS should be treated in referral centers where a multidisciplinary approach and proper oncologic resections following sarcomas guidelines recommendations are standard of care. Hence, the importance of a prompt referral even before any intervention in the event of a suspected diagnosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


