Sheikh W Jamal, Eyad Elamir, Shybin Usman, Harris Poolakundan, Maryam Almahri, Adnan Abdul Khaleq, Zidan Darwish, Eithar Musa, Anas Zayad, Bassem Al Hariri
{"title":"Mad Honey Disease: A Rare Condition in an Unlikely Locale.","authors":"Sheikh W Jamal, Eyad Elamir, Shybin Usman, Harris Poolakundan, Maryam Almahri, Adnan Abdul Khaleq, Zidan Darwish, Eithar Musa, Anas Zayad, Bassem Al Hariri","doi":"10.1155/carm/2632633","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background and Aims/Introduction:</b> Mad honey disease is caused by consuming honey containing grayanotoxanes-neurotoxins found in certain species of <i>Rhododendron</i> plants. Mad honey, derived from the nectar of these plants, can cause significant cardiovascular and neurological symptoms. While most cases are reported in regions where it is produced, extensive travel among diverse expatriate communities in various global regions is one of the factors that may contribute to cases occurring in nonendemic areas. Other factors leading to its increased demand include the global demand for its recreational and medicinal use, as well as its reputation as an aphrodisiac. Our case report on mad honey disease aims to raise awareness of this condition, highlight its clinical presentation and management, and emphasize the possibility of its occurrence outside endemic regions. <b>Case Presentation:</b> A 40-year-old Nepalese male living in Qatar presented with dizziness, hypotension, and severe bradycardia a few hours after consuming approximately 50 g of imported mad honey from Nepal. His admission ECG revealed sinus bradycardia without evidence of heart block. Initial stabilization was achieved with 0.5 mg of atropine and a norepinephrine infusion. The patient's symptoms resolved with supportive care while he was closely observed in the intensive care unit. He was discharged symptom free after 24 h. <b>Conclusion:</b> This case, to the best of our knowledge, represents the first reported incidence of mad honey disease in Qatar, emphasizing the importance of recognizing this rare condition in nonendemic areas. Proper history-taking, particularly with a focus on food and ingestion history, along with a high index of clinical suspicion, is crucial for timely diagnosis and management. While unintentional and accidental overdose and poisoning, as occurred in our case, may happen sporadically, the widespread use and import/export of mad honey necessitates stringent measures and precautions, similar to those adopted by various countries.</p>","PeriodicalId":9627,"journal":{"name":"Case Reports in Medicine","volume":"2025 ","pages":"2632633"},"PeriodicalIF":0.7000,"publicationDate":"2025-06-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12221553/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/carm/2632633","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
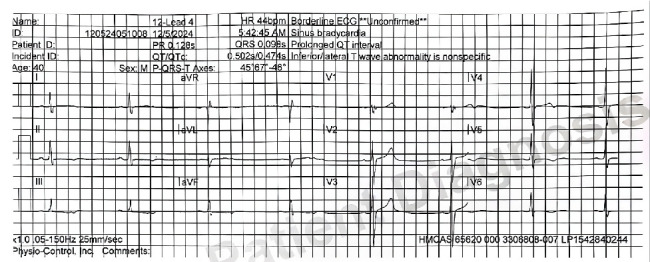
Background and Aims/Introduction: Mad honey disease is caused by consuming honey containing grayanotoxanes-neurotoxins found in certain species of Rhododendron plants. Mad honey, derived from the nectar of these plants, can cause significant cardiovascular and neurological symptoms. While most cases are reported in regions where it is produced, extensive travel among diverse expatriate communities in various global regions is one of the factors that may contribute to cases occurring in nonendemic areas. Other factors leading to its increased demand include the global demand for its recreational and medicinal use, as well as its reputation as an aphrodisiac. Our case report on mad honey disease aims to raise awareness of this condition, highlight its clinical presentation and management, and emphasize the possibility of its occurrence outside endemic regions. Case Presentation: A 40-year-old Nepalese male living in Qatar presented with dizziness, hypotension, and severe bradycardia a few hours after consuming approximately 50 g of imported mad honey from Nepal. His admission ECG revealed sinus bradycardia without evidence of heart block. Initial stabilization was achieved with 0.5 mg of atropine and a norepinephrine infusion. The patient's symptoms resolved with supportive care while he was closely observed in the intensive care unit. He was discharged symptom free after 24 h. Conclusion: This case, to the best of our knowledge, represents the first reported incidence of mad honey disease in Qatar, emphasizing the importance of recognizing this rare condition in nonendemic areas. Proper history-taking, particularly with a focus on food and ingestion history, along with a high index of clinical suspicion, is crucial for timely diagnosis and management. While unintentional and accidental overdose and poisoning, as occurred in our case, may happen sporadically, the widespread use and import/export of mad honey necessitates stringent measures and precautions, similar to those adopted by various countries.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


