Muhammad Dwi Priangga, Adhitya Yudha Maulana, Yasmine Syifa Nabila Budi, Syauqi Maulana Idhar, Herbert Situmorang
{"title":"Silent Threat: Bilateral Giant Asymptomatic Endometriotic Cysts With Unilateral Sudden Rupture-A Case Report.","authors":"Muhammad Dwi Priangga, Adhitya Yudha Maulana, Yasmine Syifa Nabila Budi, Syauqi Maulana Idhar, Herbert Situmorang","doi":"10.1155/crog/1739044","DOIUrl":null,"url":null,"abstract":"<p><p>Endometriotic cysts are common, but bilateral giant endometriosis cyst with asymptomatic cases are extremely rare. Rupture is also uncommon, yet when it occurs, it can mimic appendicitis or ectopic pregnancy due to peritoneal irritation, often requiring emergency intervention. A 25-year-old woman presented with nausea, vomiting, and an enlarging abdominal lump. Ultrasonography revealed bilateral ovarian cystic masses with ground glass appearances and free subhepatic fluid. Due to worsening symptoms despite initial resuscitation, emergency exploratory laparotomy was performed. Intraoperatively, a ruptured right ovarian cyst (20 × 15 × 15 cm) with extensive adhesions to the posterior uterus, rectum, and right ovarian fossa was identified, along with a left ovarian endometriotic cyst (12 × 10 × 10 cm). The patient underwent right salpingo-oophorectomy, left cystectomy, and ureterolysis. Histopathology confirmed endometriotic cysts. Rapid surgical intervention is crucial in ruptured cysts to minimize adhesion formation and preserve fertility. Postoperatively, continuous hormonal therapy, such as oral progesterone or an intrauterine device, is recommended to decrease recurrence.</p>","PeriodicalId":9610,"journal":{"name":"Case Reports in Obstetrics and Gynecology","volume":"2025 ","pages":"1739044"},"PeriodicalIF":0.8000,"publicationDate":"2025-06-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12221541/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Obstetrics and Gynecology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/crog/1739044","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
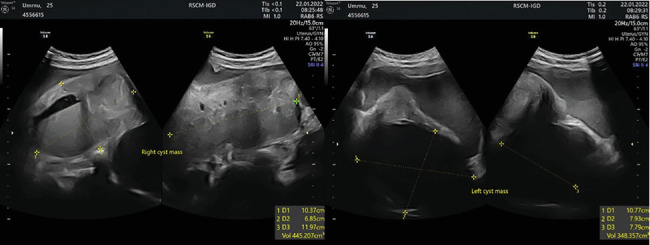
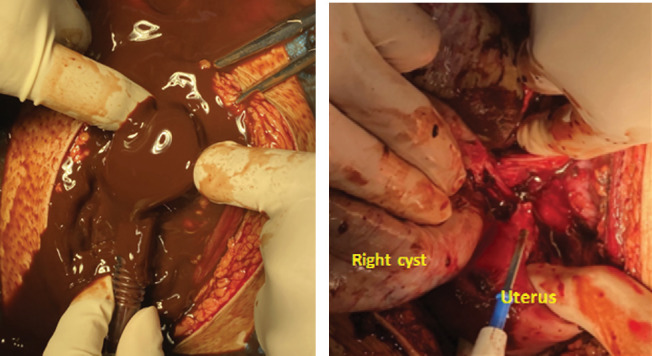
Endometriotic cysts are common, but bilateral giant endometriosis cyst with asymptomatic cases are extremely rare. Rupture is also uncommon, yet when it occurs, it can mimic appendicitis or ectopic pregnancy due to peritoneal irritation, often requiring emergency intervention. A 25-year-old woman presented with nausea, vomiting, and an enlarging abdominal lump. Ultrasonography revealed bilateral ovarian cystic masses with ground glass appearances and free subhepatic fluid. Due to worsening symptoms despite initial resuscitation, emergency exploratory laparotomy was performed. Intraoperatively, a ruptured right ovarian cyst (20 × 15 × 15 cm) with extensive adhesions to the posterior uterus, rectum, and right ovarian fossa was identified, along with a left ovarian endometriotic cyst (12 × 10 × 10 cm). The patient underwent right salpingo-oophorectomy, left cystectomy, and ureterolysis. Histopathology confirmed endometriotic cysts. Rapid surgical intervention is crucial in ruptured cysts to minimize adhesion formation and preserve fertility. Postoperatively, continuous hormonal therapy, such as oral progesterone or an intrauterine device, is recommended to decrease recurrence.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


