{"title":"Adrenal venous sampling outcomes with and without mineralocorticoid receptor antagonists in primary aldosteronism.","authors":"Sittikul Thipbumrung, Worapaka Manosroi","doi":"10.1186/s12902-025-01987-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Current guidelines recommend discontinuing mineralocorticoid receptor antagonists (MRA) at least 4 weeks before adrenal venous sampling (AVS) in primary aldosteronism (PA) to avoid interference with the lateralization index (LI). However, discontinuing MRA can cause hypertension and hypokalemia. This study aimed to evaluate the impact of continuing MRA use prior to AVS.</p><p><strong>Methods: </strong>A 5-year retrospective cohort study of patients aged ≥ 18 with PA who underwent successful AVS was conducted. Patients were divided into two groups: those who continued MRA during AVS and those who discontinued it for at least 4 weeks prior. Outcomes included differences in LI, plasma renin activity (PRA) levels before AVS, and post-adrenalectomy outcomes. Linear regression analysis clustered by subtypes of PA was used to adjust for confounders.</p><p><strong>Results: </strong>A total of 66 patients were included, with 30 (45.5%) in the continued MRA group and 36 (54.5%) in the discontinued MRA group. After adjustment for confounders, PRA levels before AVS showed no significant difference between the groups (β-coefficient 0.5, 95% CI -2.0 to 3.0; p = 0.239) and there was no significant difference in the LI between the continued and discontinued MRA groups (β-coefficient 7.9, 95% CI -27.8 to 43.7; p = 0.216). Clinical and biochemical success after unilateral adrenalectomy were similar between the two groups (p = 0.141 and p = 0.596, respectively).</p><p><strong>Conclusion: </strong>Continuing MRA prior to AVS did not appear to affect the interpretation of lateralization and may be a reasonable option for patients at high risk of complications from MRA withdrawal. Further prospective studies are needed to confirm these observations.</p>","PeriodicalId":9152,"journal":{"name":"BMC Endocrine Disorders","volume":"25 1","pages":"165"},"PeriodicalIF":3.3000,"publicationDate":"2025-07-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12219769/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Endocrine Disorders","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12902-025-01987-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Current guidelines recommend discontinuing mineralocorticoid receptor antagonists (MRA) at least 4 weeks before adrenal venous sampling (AVS) in primary aldosteronism (PA) to avoid interference with the lateralization index (LI). However, discontinuing MRA can cause hypertension and hypokalemia. This study aimed to evaluate the impact of continuing MRA use prior to AVS.
Methods: A 5-year retrospective cohort study of patients aged ≥ 18 with PA who underwent successful AVS was conducted. Patients were divided into two groups: those who continued MRA during AVS and those who discontinued it for at least 4 weeks prior. Outcomes included differences in LI, plasma renin activity (PRA) levels before AVS, and post-adrenalectomy outcomes. Linear regression analysis clustered by subtypes of PA was used to adjust for confounders.
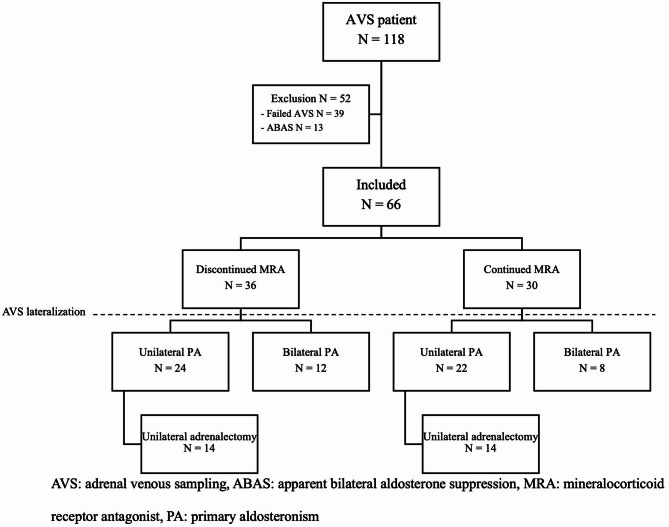
Results: A total of 66 patients were included, with 30 (45.5%) in the continued MRA group and 36 (54.5%) in the discontinued MRA group. After adjustment for confounders, PRA levels before AVS showed no significant difference between the groups (β-coefficient 0.5, 95% CI -2.0 to 3.0; p = 0.239) and there was no significant difference in the LI between the continued and discontinued MRA groups (β-coefficient 7.9, 95% CI -27.8 to 43.7; p = 0.216). Clinical and biochemical success after unilateral adrenalectomy were similar between the two groups (p = 0.141 and p = 0.596, respectively).
Conclusion: Continuing MRA prior to AVS did not appear to affect the interpretation of lateralization and may be a reasonable option for patients at high risk of complications from MRA withdrawal. Further prospective studies are needed to confirm these observations.
期刊介绍:
BMC Endocrine Disorders is an open access, peer-reviewed journal that considers articles on all aspects of the prevention, diagnosis and management of endocrine disorders, as well as related molecular genetics, pathophysiology, and epidemiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


