Kelvin Cheuk Man Cheung, Gavin Tin Chun Cheung, Ka Man Cheung, James Chung Hang Chow, Kwok Hung Au
{"title":"Optimal radiotherapy dose and fractionation for stereotactic radiotherapy in excised brain metastases.","authors":"Kelvin Cheuk Man Cheung, Gavin Tin Chun Cheung, Ka Man Cheung, James Chung Hang Chow, Kwok Hung Au","doi":"10.3857/roj.2024.00556","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Stereotactic radiotherapy (SRT) is an important adjunctive treatment after excision of brain metastases. We investigated efficacy and safety outcomes of such treatment and the impact of radiotherapy dose fractionations in a real-world multi-center cohort.</p><p><strong>Materials and methods: </strong>All patients who received resection cavity SRT between 2018-2022 were identified from institutional databases of two tertiary oncology centers. Patient and treatment characteristics were summarized using descriptive statistics. Local control rate (LCR), distant brain control rate (DBCR), and overall survival (OS) were estimated. Prognostic factors were investigated using univariate/multivariate Cox regression. The incidence of radiation necrosis (RN) was reported.</p><p><strong>Results: </strong>Sixty-five cavities were analyzed. The most used SRT prescription was 30 Gy/5 fractions. One-year LCR, DBCR, and OS were 69.0%, 51.9%, and 71.0%, respectively. BED10 (biological effective dose using α/β ratio of 10) was a significant factor for improved local control on both univariate (hazard ratio [HR], 0.862; 95% confidence interval [CI], 0.787 to 0.944; p = 0.001) and multivariate analysis (HR, 0.890; 95% CI, 0.803 to 0.986; p = 0.026). Cavities prescribed BED10 ≥45 Gy had superior local control than those prescribed BED10 <45 Gy (p = 0.002). The rate of RN was 6.2%. Single-fraction treatment had higher rates of RN (p = 0.030). There was no significant difference in LCR between single-fraction and fractionated subgroups in cavities with BED10 ≥45 Gy (p = 0.542).</p><p><strong>Conclusion: </strong>BED10 independently predicts LCR in resection cavity SRT. Fractionated treatment is associated with a lower risk of RN and did not appear to compromise outcomes as long as prescription BED10 ≥45 Gy.</p>","PeriodicalId":94184,"journal":{"name":"Radiation oncology journal","volume":"43 2","pages":"79-87"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12215343/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiation oncology journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3857/roj.2024.00556","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/11 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Stereotactic radiotherapy (SRT) is an important adjunctive treatment after excision of brain metastases. We investigated efficacy and safety outcomes of such treatment and the impact of radiotherapy dose fractionations in a real-world multi-center cohort.
Materials and methods: All patients who received resection cavity SRT between 2018-2022 were identified from institutional databases of two tertiary oncology centers. Patient and treatment characteristics were summarized using descriptive statistics. Local control rate (LCR), distant brain control rate (DBCR), and overall survival (OS) were estimated. Prognostic factors were investigated using univariate/multivariate Cox regression. The incidence of radiation necrosis (RN) was reported.
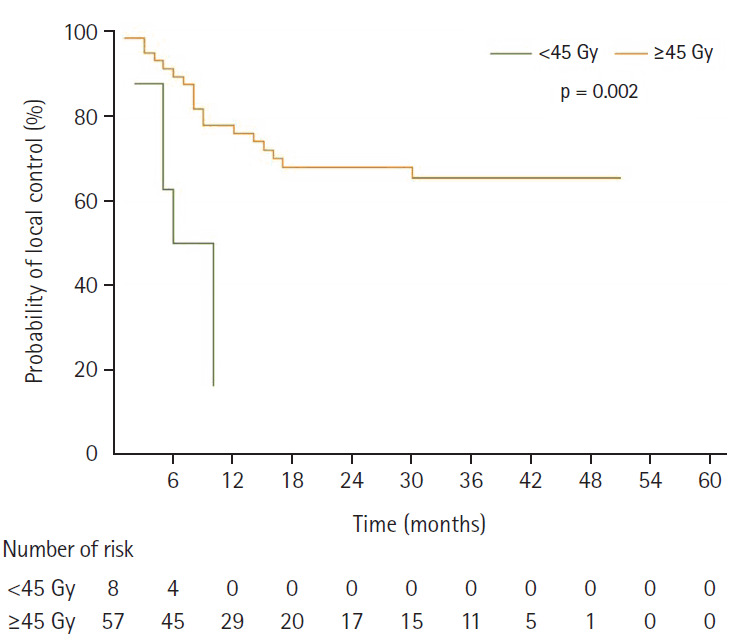
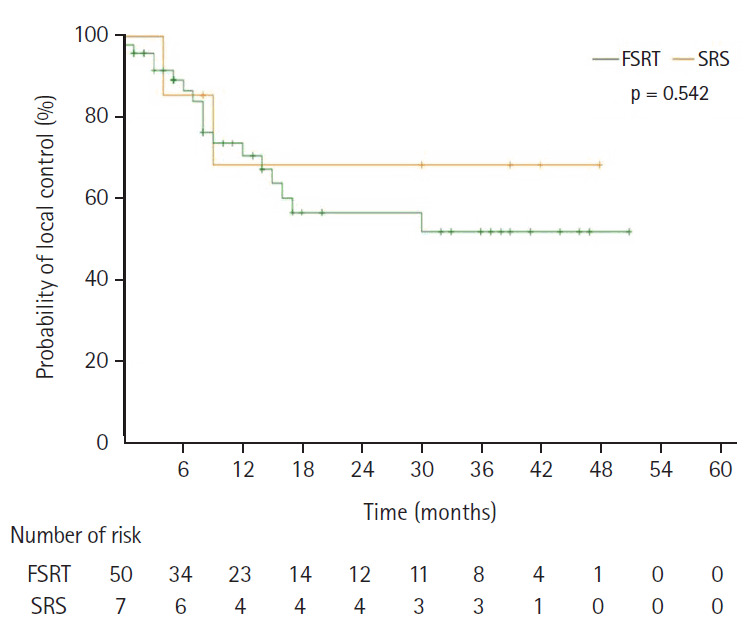
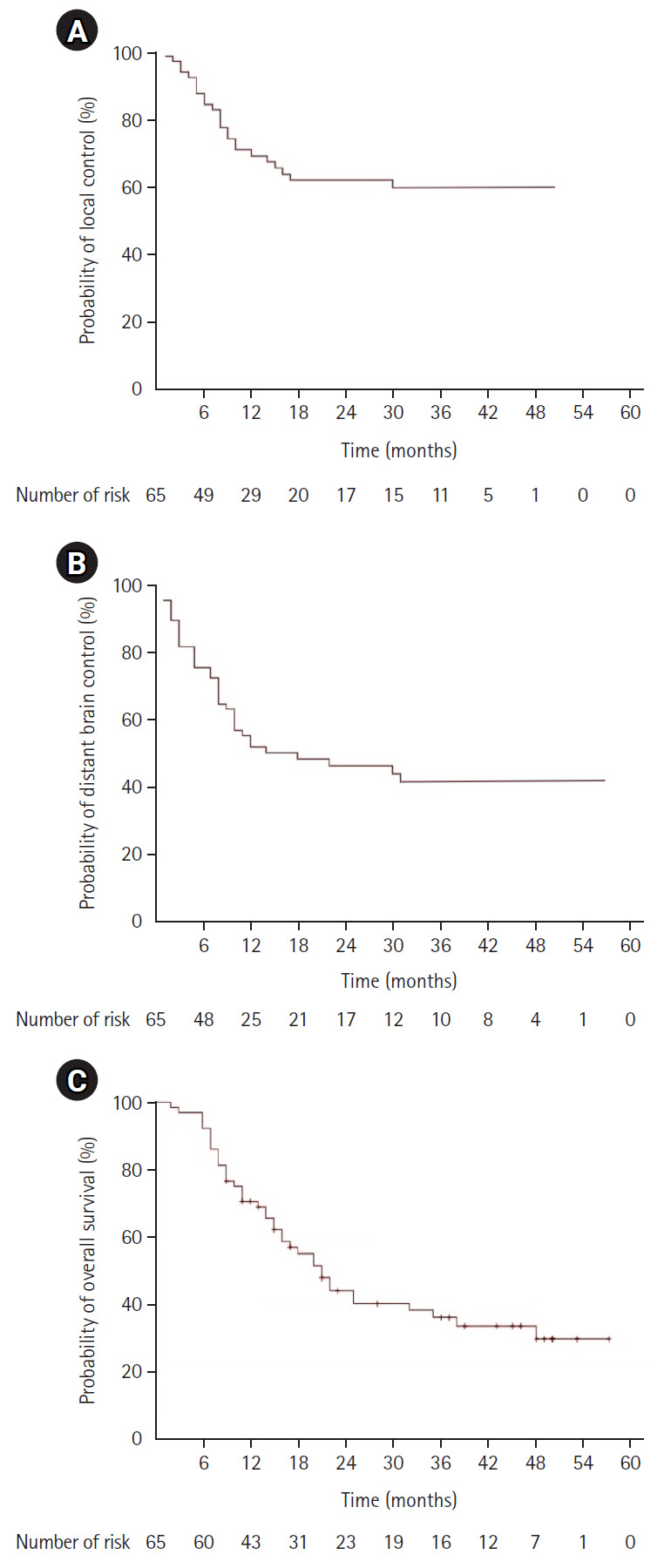
Results: Sixty-five cavities were analyzed. The most used SRT prescription was 30 Gy/5 fractions. One-year LCR, DBCR, and OS were 69.0%, 51.9%, and 71.0%, respectively. BED10 (biological effective dose using α/β ratio of 10) was a significant factor for improved local control on both univariate (hazard ratio [HR], 0.862; 95% confidence interval [CI], 0.787 to 0.944; p = 0.001) and multivariate analysis (HR, 0.890; 95% CI, 0.803 to 0.986; p = 0.026). Cavities prescribed BED10 ≥45 Gy had superior local control than those prescribed BED10 <45 Gy (p = 0.002). The rate of RN was 6.2%. Single-fraction treatment had higher rates of RN (p = 0.030). There was no significant difference in LCR between single-fraction and fractionated subgroups in cavities with BED10 ≥45 Gy (p = 0.542).
Conclusion: BED10 independently predicts LCR in resection cavity SRT. Fractionated treatment is associated with a lower risk of RN and did not appear to compromise outcomes as long as prescription BED10 ≥45 Gy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


