Pervin Hurmuz, Alper Kahvecioglu, Gokhan Ozyigit, Omer Dizdar, Mustafa Cengiz
{"title":"Definitive radiotherapy for unresectable extrahepatic cholangiocarcinoma: is it time for an update?","authors":"Pervin Hurmuz, Alper Kahvecioglu, Gokhan Ozyigit, Omer Dizdar, Mustafa Cengiz","doi":"10.3857/roj.2024.00437","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>For patients with unresectable extrahepatic cholangiocarcinoma, radiotherapy (RT) is the definitive treatment. In this study, we aimed to evaluate the role of two different RT techniques for definitive treatment of unresectable extrahepatic cholangiocarcinoma.</p><p><strong>Materials and methods: </strong>Eighteen patients with unresectable extrahepatic cholangiocarcinoma treated with either conventionally fractionated radiotherapy (CFRT) or stereotactic body radiotherapy (SBRT) were evaluated retrospectively. Patients treated with CFRT also received elective nodal irradiation (ENI) in addition to the primary tumor.</p><p><strong>Results: </strong>Median doses of CFRT and SBRT were 50.4 Gy (range, 45 to 59.4) in 25-33 fractions and 37.5 Gy (range, 27.5 to 50) in 3-5 fractions, respectively. Median follow-up was 22 months (range, 7 to 138). During follow-up, local failure occured in one patient (12.5%) in the SBRT group and six patients (60.0%) in the CFRT group (p = 0.041). On the other hand, regional failure occured in five patients (62.5%) in the SBRT group and in two patients (20.0%) in the CFRT group (p = 0.047). Two-year overall survival (OS), local-regional failure-free survival (LRFFS), and distant metastasis-free survival (DMFS) rates were 35%, 30%, and 24%, respectively. Younger age (≤55 years) was associated with better OS, LRFFS, and DMFS. None of the patients experienced ≥grade 3 acute or late toxicity.</p><p><strong>Conclusion: </strong>While SBRT may provide better local tumor control compared to CFRT, the absence of ENI can result in increased regional recurrences. Hence, conducting prospective studies to examine the safety and efficacy of integrating hypofractionated ENI into SBRT is warranted.</p>","PeriodicalId":94184,"journal":{"name":"Radiation oncology journal","volume":"43 2","pages":"57-62"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12215330/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiation oncology journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3857/roj.2024.00437","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/25 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: For patients with unresectable extrahepatic cholangiocarcinoma, radiotherapy (RT) is the definitive treatment. In this study, we aimed to evaluate the role of two different RT techniques for definitive treatment of unresectable extrahepatic cholangiocarcinoma.
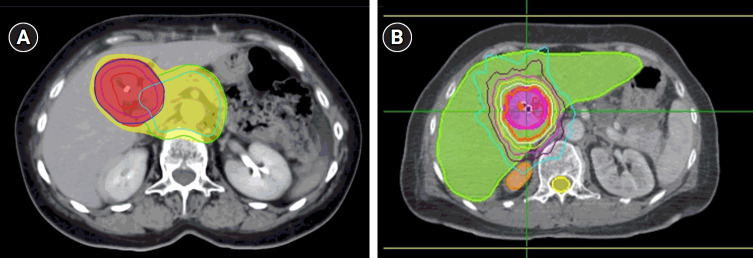
Materials and methods: Eighteen patients with unresectable extrahepatic cholangiocarcinoma treated with either conventionally fractionated radiotherapy (CFRT) or stereotactic body radiotherapy (SBRT) were evaluated retrospectively. Patients treated with CFRT also received elective nodal irradiation (ENI) in addition to the primary tumor.
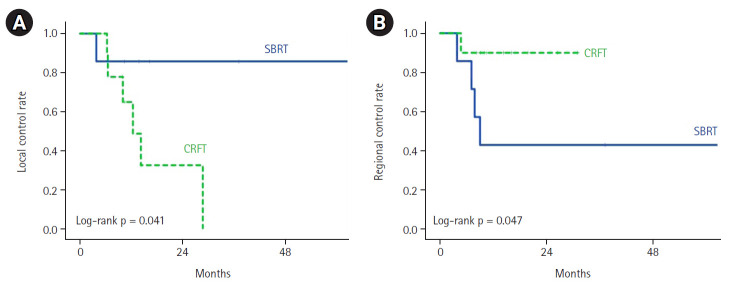
Results: Median doses of CFRT and SBRT were 50.4 Gy (range, 45 to 59.4) in 25-33 fractions and 37.5 Gy (range, 27.5 to 50) in 3-5 fractions, respectively. Median follow-up was 22 months (range, 7 to 138). During follow-up, local failure occured in one patient (12.5%) in the SBRT group and six patients (60.0%) in the CFRT group (p = 0.041). On the other hand, regional failure occured in five patients (62.5%) in the SBRT group and in two patients (20.0%) in the CFRT group (p = 0.047). Two-year overall survival (OS), local-regional failure-free survival (LRFFS), and distant metastasis-free survival (DMFS) rates were 35%, 30%, and 24%, respectively. Younger age (≤55 years) was associated with better OS, LRFFS, and DMFS. None of the patients experienced ≥grade 3 acute or late toxicity.
Conclusion: While SBRT may provide better local tumor control compared to CFRT, the absence of ENI can result in increased regional recurrences. Hence, conducting prospective studies to examine the safety and efficacy of integrating hypofractionated ENI into SBRT is warranted.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


