Development and validation of a novel clinical-radiological-pathological scoring system for preoperative prediction of extraprostatic extension in prostate cancer: a multicenter retrospective study.
{"title":"Development and validation of a novel clinical-radiological-pathological scoring system for preoperative prediction of extraprostatic extension in prostate cancer: a multicenter retrospective study.","authors":"Liqin Yang, Pengfei Jin, Ximing Wang, Zhiping Li, Huijing Xu, Yongsheng Zhang, Feng Cui","doi":"10.1186/s40644-025-00905-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To develop and validate a multimodal scoring system integrating clinical, radiological, and pathological variables to preoperatively predict extraprostatic extension (EPE) in prostate cancer (PCa).</p><p><strong>Methods: </strong>This retrospective study included 667 PCa patients divided into a derivation cohort and two validation cohorts. Evaluated parameters comprised prostate-specific antigen density (PSAD), curvilinear contact length (CCL), lesion longest diameter (LD), National Cancer Institute EPE grade (NCI_EPE), International Society of Urological Pathology grade (ISUP), and other relevant variables. Independent predictors were identified through univariate and multivariate regression analysis to construct a logistic model. Coefficients from this model were then weighted to establish a scoring system. The predictive performance of the NCI_EPE, logistic model, and scoring system was systematically evaluated and compared. Finally, the scoring system was stratified into four distinct risk categories.</p><p><strong>Results: </strong>Multivariate analysis identified NCI_EPE, PSAD, CCL/LD, and ISUP as independent predictors of EPE. In the derivation and validation cohorts, the scoring system demonstrated robust predictive accuracy for EPE, with AUCs of 0.849, 0.830, and 0.847, respectively. These values outperformed the NCI_EPE (Derivation cohort: 0.849 vs. 0.750, P < 0.003, Validation cohort 1: 0.830 vs. 0.736, P = 0.138, Validation cohort 2: 0.837 vs. 0.715, P = 0.003) and were comparable to the logistic model (Derivation cohort: 0.849 vs. 0.860, P = 0.228, Validation cohort 1: 0.830 vs. 0.849, P = 0.711, Validation cohort 2: 0.837 vs. 0.843, P = 0.738). Decision curve analysis revealed higher net clinical benefit for both the scoring system and logistic model compared to the NCI_EPE. Risk stratification using the scoring system categorized patients into four tiers: low (0-3), intermediate-low (4-6), intermediate-high (7-9), and high risk (10-12) with corresponding mean EPE probabilities of 9.9%, 26.0%, 52.0%, and 85.0%. These probabilities closely aligned with observed pT3 incidences in the derivation and validation cohorts.</p><p><strong>Conclusions: </strong>The scoring system provides enhanced predictive accuracy for EPE, preoperatively stratifying patients into distinct risk categories to facilitate personalized therapeutic strategies.</p>","PeriodicalId":9548,"journal":{"name":"Cancer Imaging","volume":"25 1","pages":"83"},"PeriodicalIF":3.5000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12220475/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Imaging","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40644-025-00905-w","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To develop and validate a multimodal scoring system integrating clinical, radiological, and pathological variables to preoperatively predict extraprostatic extension (EPE) in prostate cancer (PCa).
Methods: This retrospective study included 667 PCa patients divided into a derivation cohort and two validation cohorts. Evaluated parameters comprised prostate-specific antigen density (PSAD), curvilinear contact length (CCL), lesion longest diameter (LD), National Cancer Institute EPE grade (NCI_EPE), International Society of Urological Pathology grade (ISUP), and other relevant variables. Independent predictors were identified through univariate and multivariate regression analysis to construct a logistic model. Coefficients from this model were then weighted to establish a scoring system. The predictive performance of the NCI_EPE, logistic model, and scoring system was systematically evaluated and compared. Finally, the scoring system was stratified into four distinct risk categories.
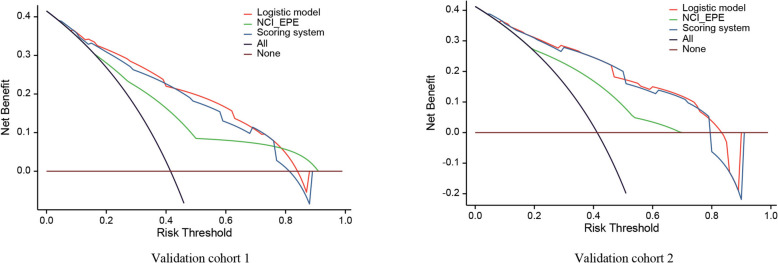
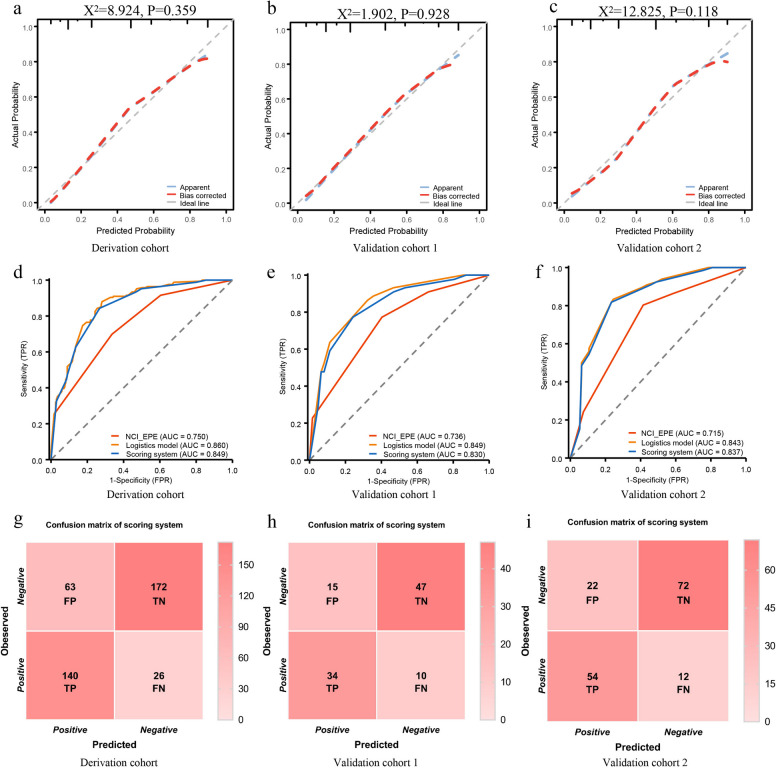
Results: Multivariate analysis identified NCI_EPE, PSAD, CCL/LD, and ISUP as independent predictors of EPE. In the derivation and validation cohorts, the scoring system demonstrated robust predictive accuracy for EPE, with AUCs of 0.849, 0.830, and 0.847, respectively. These values outperformed the NCI_EPE (Derivation cohort: 0.849 vs. 0.750, P < 0.003, Validation cohort 1: 0.830 vs. 0.736, P = 0.138, Validation cohort 2: 0.837 vs. 0.715, P = 0.003) and were comparable to the logistic model (Derivation cohort: 0.849 vs. 0.860, P = 0.228, Validation cohort 1: 0.830 vs. 0.849, P = 0.711, Validation cohort 2: 0.837 vs. 0.843, P = 0.738). Decision curve analysis revealed higher net clinical benefit for both the scoring system and logistic model compared to the NCI_EPE. Risk stratification using the scoring system categorized patients into four tiers: low (0-3), intermediate-low (4-6), intermediate-high (7-9), and high risk (10-12) with corresponding mean EPE probabilities of 9.9%, 26.0%, 52.0%, and 85.0%. These probabilities closely aligned with observed pT3 incidences in the derivation and validation cohorts.
Conclusions: The scoring system provides enhanced predictive accuracy for EPE, preoperatively stratifying patients into distinct risk categories to facilitate personalized therapeutic strategies.
目的:开发和验证一种综合临床、影像学和病理变量的多模式评分系统,用于术前预测前列腺癌(PCa)的前列腺外展(EPE)。方法:本回顾性研究纳入667例PCa患者,分为衍生队列和两个验证队列。评估参数包括前列腺特异性抗原密度(PSAD)、曲线接触长度(CCL)、病变最长直径(LD)、美国国家癌症研究所EPE分级(NCI_EPE)、国际泌尿病理学会分级(ISUP)和其他相关变量。通过单变量和多变量回归分析确定独立预测因子,构建logistic模型。然后对该模型的系数进行加权以建立评分系统。对NCI_EPE、logistic模型和评分系统的预测性能进行系统评价和比较。最后,将评分系统分为四个不同的风险类别。结果:多因素分析发现NCI_EPE、PSAD、CCL/LD和ISUP是EPE的独立预测因子。在推导组和验证组中,该评分系统对EPE的预测准确率较高,auc分别为0.849、0.830和0.847。这些值优于NCI_EPE(衍生队列:0.849 vs. 0.750, P)。结论:评分系统提高了EPE的预测准确性,术前将患者分为不同的风险类别,以促进个性化的治疗策略。
Cancer ImagingONCOLOGY-RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING
CiteScore
7.00
自引率
0.00%
发文量
66
审稿时长
>12 weeks
期刊介绍:
Cancer Imaging is an open access, peer-reviewed journal publishing original articles, reviews and editorials written by expert international radiologists working in oncology.
The journal encompasses CT, MR, PET, ultrasound, radionuclide and multimodal imaging in all kinds of malignant tumours, plus new developments, techniques and innovations. Topics of interest include:
Breast Imaging
Chest
Complications of treatment
Ear, Nose & Throat
Gastrointestinal
Hepatobiliary & Pancreatic
Imaging biomarkers
Interventional
Lymphoma
Measurement of tumour response
Molecular functional imaging
Musculoskeletal
Neuro oncology
Nuclear Medicine
Paediatric.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


