{"title":"Integration of clinical and serological biomarkers in a nomogram for predicting interstitial lung disease in idiopathic inflammatory myopathies.","authors":"Zhixia Wang, Jingyun Zhang, Jin Li, Xiaona Mao, Yangyang Li, Dekun Wang, Wenpeng Ge, Jingzhan Li, Changhua Liang, Zhiqiang Zhang","doi":"10.1186/s41927-025-00534-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Idiopathic inflammatory myopathies (IIM) are a diverse group of autoimmune diseases characterized primarily by muscle weakness and systemic involvement, which can include interstitial lung disease (ILD). ILD is a serious complication in IIM, significantly affecting patient prognosis and quality of life. Early identification of IIM patients at risk for developing ILD is crucial for timely intervention and personalized treatment, yet the factors contributing to this risk remain inadequately defined.</p><p><strong>Methods: </strong>This retrospective study analyzed medical records of 130 patients with IIM from the First Affiliated Hospital of Xinxiang Medical University, China, between August 2018 and July 2023. Patients were categorized into two groups: IIM with interstitial lung disease (IIM-ILD, n = 75) and IIM without ILD (n = 55). We collected and analyzed demographic, clinical, and laboratory data, including specific autoantibody tests. Multivariate logistic regression identified independent predictors of ILD, and a nomogram was developed to evaluate ILD risk based on significant factors.</p><p><strong>Results: </strong>This retrospective study analyzed 130 patients with IIM, including 75 with interstitial lung disease and 55 without ILD. The IIM-ILD group was significantly older (58.4 vs. 48.3, p = 0.052) and had higher frequencies of respiratory symptoms including dyspnea (61.3% vs. 14.9%, p < 0.001) and cough (54.7% vs. 10.9%, p < 0.001). Key laboratory differences included elevated ESR (26.5 vs. 10.0 mm/H, p < 0.001), CRP (3.44 vs. 1.64 mmol/L, p = 0.013), and IgG (12.5 vs. 10.9 g/L, p = 0.006), along with lower ALT (29.0 vs. 44.0 U/L, p = 0.001) and AST (32.0 vs. 45.0 U/L, p = 0.021) in the IIM-ILD group. Anti-Jo-1 antibodies were more prevalent in IIM-ILD patients (18.7% vs. 5.5%, p = 0.027). Multivariate analysis identified ESR (OR = 1.063, 95% CI:1.012-1.117, p = 0.015), AST (OR = 0.985, 95% CI:0.970-1.000, p = 0.047), and IgG (OR = 1.191, 95% CI:1.025-1.383, p = 0.022) as independent predictors. These factors, combined with dyspnea and anti-Jo-1 status, were incorporated into a predictive nomogram model. The nomogram demonstrated excellent discrimination (AUC = 0.891, 95% CI:0.836-0.947) with sensitivity of 79.7% and specificity of 82.6%. Calibration curves showed good agreement between predicted and observed outcomes (Hosmer-Lemeshow test, p = 0.779). Decision curve analysis confirmed the model's clinical utility across a wide range of threshold probabilities. This comprehensive model provides clinicians with a practical tool for early identification of IIM patients at high risk for ILD development.</p><p><strong>Conclusion: </strong>Elevated ESR and CRP levels, in conjunction with lower AST levels, alongside the presence of anti-Jo-1 antibodies and the manifestation of dyspnea are significant biomarkers associated with the risk of developing IIM-ILD. This predictive model enhances early diagnostic capabilities and facilitates risk stratification, thereby informing clinical decision-making. However, further validation in larger, multicenter cohorts is warranted to corroborate the model's predictive accuracy and to optimize its clinical utility.</p>","PeriodicalId":9150,"journal":{"name":"BMC Rheumatology","volume":"9 1","pages":"73"},"PeriodicalIF":2.5000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12219061/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41927-025-00534-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Idiopathic inflammatory myopathies (IIM) are a diverse group of autoimmune diseases characterized primarily by muscle weakness and systemic involvement, which can include interstitial lung disease (ILD). ILD is a serious complication in IIM, significantly affecting patient prognosis and quality of life. Early identification of IIM patients at risk for developing ILD is crucial for timely intervention and personalized treatment, yet the factors contributing to this risk remain inadequately defined.
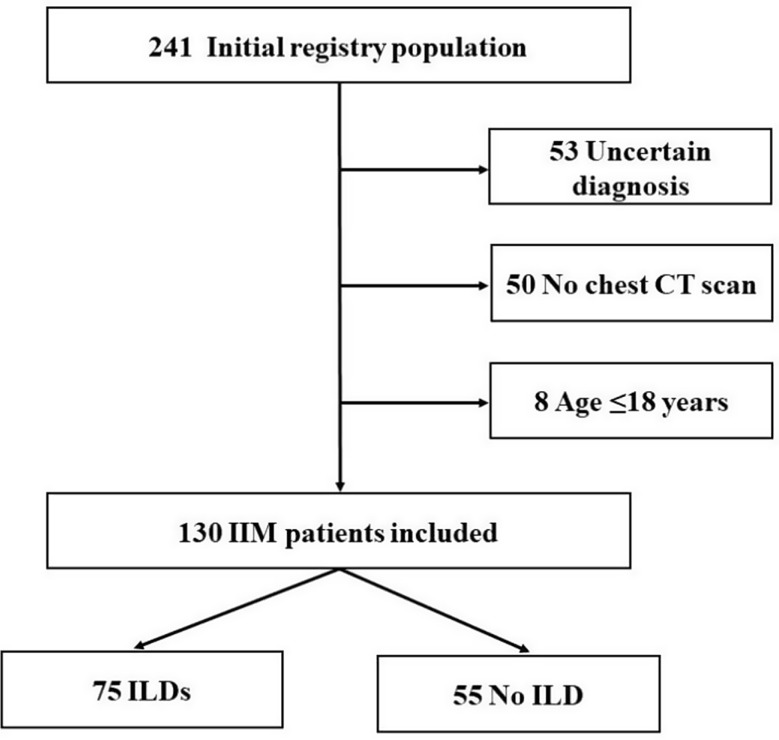
Methods: This retrospective study analyzed medical records of 130 patients with IIM from the First Affiliated Hospital of Xinxiang Medical University, China, between August 2018 and July 2023. Patients were categorized into two groups: IIM with interstitial lung disease (IIM-ILD, n = 75) and IIM without ILD (n = 55). We collected and analyzed demographic, clinical, and laboratory data, including specific autoantibody tests. Multivariate logistic regression identified independent predictors of ILD, and a nomogram was developed to evaluate ILD risk based on significant factors.
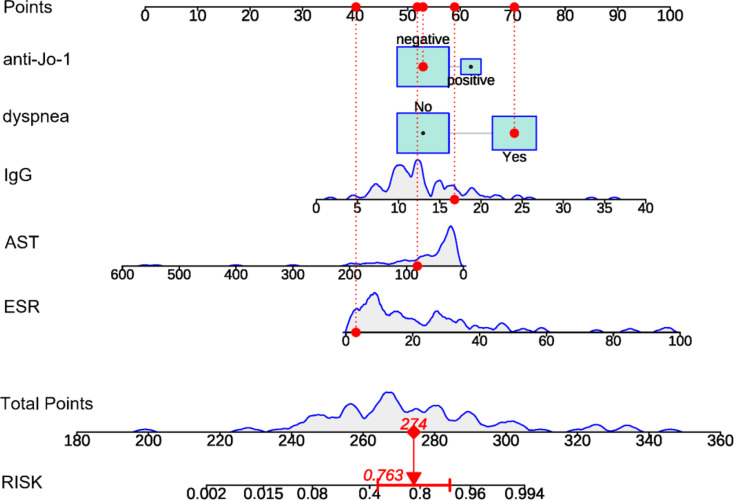
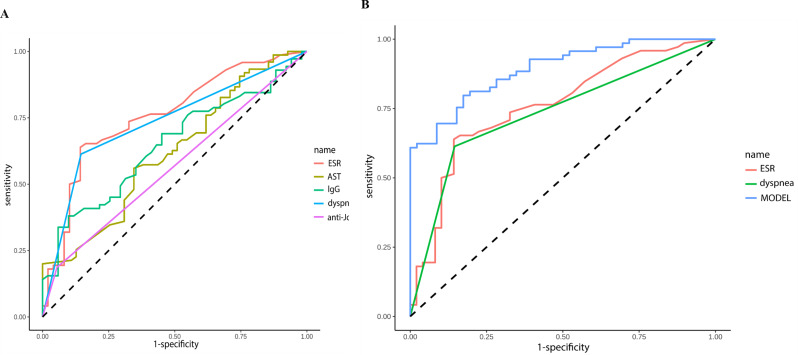
Results: This retrospective study analyzed 130 patients with IIM, including 75 with interstitial lung disease and 55 without ILD. The IIM-ILD group was significantly older (58.4 vs. 48.3, p = 0.052) and had higher frequencies of respiratory symptoms including dyspnea (61.3% vs. 14.9%, p < 0.001) and cough (54.7% vs. 10.9%, p < 0.001). Key laboratory differences included elevated ESR (26.5 vs. 10.0 mm/H, p < 0.001), CRP (3.44 vs. 1.64 mmol/L, p = 0.013), and IgG (12.5 vs. 10.9 g/L, p = 0.006), along with lower ALT (29.0 vs. 44.0 U/L, p = 0.001) and AST (32.0 vs. 45.0 U/L, p = 0.021) in the IIM-ILD group. Anti-Jo-1 antibodies were more prevalent in IIM-ILD patients (18.7% vs. 5.5%, p = 0.027). Multivariate analysis identified ESR (OR = 1.063, 95% CI:1.012-1.117, p = 0.015), AST (OR = 0.985, 95% CI:0.970-1.000, p = 0.047), and IgG (OR = 1.191, 95% CI:1.025-1.383, p = 0.022) as independent predictors. These factors, combined with dyspnea and anti-Jo-1 status, were incorporated into a predictive nomogram model. The nomogram demonstrated excellent discrimination (AUC = 0.891, 95% CI:0.836-0.947) with sensitivity of 79.7% and specificity of 82.6%. Calibration curves showed good agreement between predicted and observed outcomes (Hosmer-Lemeshow test, p = 0.779). Decision curve analysis confirmed the model's clinical utility across a wide range of threshold probabilities. This comprehensive model provides clinicians with a practical tool for early identification of IIM patients at high risk for ILD development.
Conclusion: Elevated ESR and CRP levels, in conjunction with lower AST levels, alongside the presence of anti-Jo-1 antibodies and the manifestation of dyspnea are significant biomarkers associated with the risk of developing IIM-ILD. This predictive model enhances early diagnostic capabilities and facilitates risk stratification, thereby informing clinical decision-making. However, further validation in larger, multicenter cohorts is warranted to corroborate the model's predictive accuracy and to optimize its clinical utility.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


