Siyu Dai, Ming Yang, Chun Ting Au, Nobel Tsz Kin Yuen, Yuzheng Zhang, Agatha Tang, Michelle Wai Ling Yu, Albert Martin Li, Kate Ching Ching Chan
{"title":"Supine position-related obstructive sleep apnea in children: insights from the Childhood Adenotonsillectomy Trial.","authors":"Siyu Dai, Ming Yang, Chun Ting Au, Nobel Tsz Kin Yuen, Yuzheng Zhang, Agatha Tang, Michelle Wai Ling Yu, Albert Martin Li, Kate Ching Ching Chan","doi":"10.1007/s11325-025-03393-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This study aimed to examine the effectiveness of adenotonsillectomy (AT) among pediatric obstructive sleep apnea (OSA) patients with and without supine position-related OSA (POSA) and explore the stability of this subtype over time.</p><p><strong>Methods: </strong>Data from the Childhood Adenotonsillectomy Trial (CHAT) were analyzed. Children with OSA were randomized to early AT (EAT) or watchful waiting with supportive care (WWSC). Polysomnographic and health outcomes were assessed at baseline and 7 months. POSA was defined as a supine obstructive apnea-hypopnea index (OAHI) ≥ 2× non-supine OAHI, with ≥ 30 min spent in each position.</p><p><strong>Results: </strong>Among 354 patients (mean age: 6.97 ± 1.39 years; male: 48.1%), 47.2% had POSA at baseline. Compared to non-POSA, children with POSA exhibited lower baseline OAHI [3.77 (2.48, 7.71) vs. 5.42 (3.03, 9.47) events/h, p = 0.006], longer rapid eye movement (REM) sleep in the supine position (p = 0.05), shorter REM sleep in non-supine position (p = 0.005), and fewer allergic conditions (37.7% vs. 48.4%, p = 0.05). Generalized linear models showed AHI reduction was associated with randomization grouping (p < 0.001) but not POSA status (p = 0.10). Our restricted cubic splines further supported this finding. Notably, in the WWSC group, POSA classification changed for half of the patients over 7 months, with changes in non-supine OAHI as a significant indicator.</p><p><strong>Conclusion: </strong>AT is effective in managing childhood OSA regardless of POSA status. The observed dynamic nature of POSA warrants future research into its pathophysiology and natural history.</p><p><strong>Clinical trial registration: </strong>Childhood Adenotonsillectomy Study for Children with OSAS (CHAT), Clinical Trial Identifier NCT00560859.</p>","PeriodicalId":520777,"journal":{"name":"Sleep & breathing = Schlaf & Atmung","volume":"29 4","pages":"230"},"PeriodicalIF":2.0000,"publicationDate":"2025-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12209019/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Sleep & breathing = Schlaf & Atmung","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s11325-025-03393-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: This study aimed to examine the effectiveness of adenotonsillectomy (AT) among pediatric obstructive sleep apnea (OSA) patients with and without supine position-related OSA (POSA) and explore the stability of this subtype over time.
Methods: Data from the Childhood Adenotonsillectomy Trial (CHAT) were analyzed. Children with OSA were randomized to early AT (EAT) or watchful waiting with supportive care (WWSC). Polysomnographic and health outcomes were assessed at baseline and 7 months. POSA was defined as a supine obstructive apnea-hypopnea index (OAHI) ≥ 2× non-supine OAHI, with ≥ 30 min spent in each position.
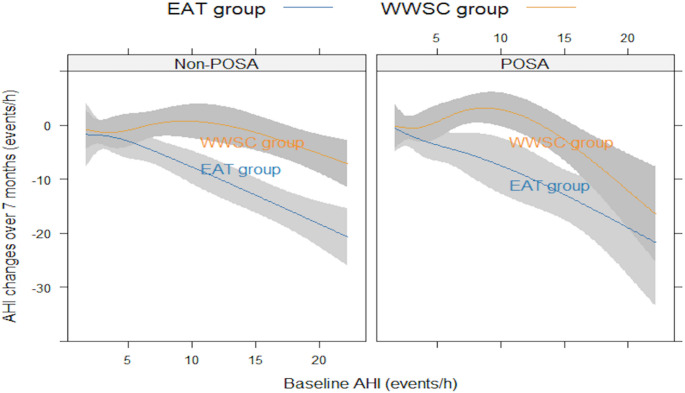
Results: Among 354 patients (mean age: 6.97 ± 1.39 years; male: 48.1%), 47.2% had POSA at baseline. Compared to non-POSA, children with POSA exhibited lower baseline OAHI [3.77 (2.48, 7.71) vs. 5.42 (3.03, 9.47) events/h, p = 0.006], longer rapid eye movement (REM) sleep in the supine position (p = 0.05), shorter REM sleep in non-supine position (p = 0.005), and fewer allergic conditions (37.7% vs. 48.4%, p = 0.05). Generalized linear models showed AHI reduction was associated with randomization grouping (p < 0.001) but not POSA status (p = 0.10). Our restricted cubic splines further supported this finding. Notably, in the WWSC group, POSA classification changed for half of the patients over 7 months, with changes in non-supine OAHI as a significant indicator.
Conclusion: AT is effective in managing childhood OSA regardless of POSA status. The observed dynamic nature of POSA warrants future research into its pathophysiology and natural history.
Clinical trial registration: Childhood Adenotonsillectomy Study for Children with OSAS (CHAT), Clinical Trial Identifier NCT00560859.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


