Relationship Between Improvements in Glycemic Control and Risk of Pregnancy Complications in Patients With Diabetes Mellitus: Metaregression Analysis of Randomized Controlled Trials of Intensive Glucose Management.
{"title":"Relationship Between Improvements in Glycemic Control and Risk of Pregnancy Complications in Patients With Diabetes Mellitus: Metaregression Analysis of Randomized Controlled Trials of Intensive Glucose Management.","authors":"Satoru Kodama, Kazuya Fujihara, Noriko Yagyuuda, Yoko Yachi, Chika Horikawa, Yasunaga Takeda, Sakiko Yoshizawa Morikawa, Takaho Yamada, Kiminori Kato, Yoshimi Nakagawa, Shiro Tanaka, Hitoshi Shimano, Hirohito Sone","doi":"10.1155/jdr/3490884","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> It remains unknown whether improvements in prognosis of pregnancy in patients with diabetes mellitus are dependent on glycemic control (GC). This metaregression analysis was aimed at exploring the relationships between the improvements in GC. <b>Methods:</b> Using Embase and MEDLINE (from Jan. 1, 1950, to Apr. 29, 2024), we searched for randomized controlled trials of intensive glucose management in pregnant women with gestational, pregestational, or overt diabetes mellitus, in which the blood glucose level using any GC indicator and the incidence of any adverse maternal and/or fetal outcome were compared between two groups with different intensities of glucose management. Relative risks (RRs) of individual adverse outcomes were regressed on the reductions in individual GC indicators. <b>Results:</b> We examined the dose-response relationship between reductions in four GC indicators (hemoglobin A1c (A1C), fasting plasma glucose (FPG), 2-h postprandial glucose, and mean blood glucose) and 14 adverse pregnancy outcomes in 62 eligible trials. Reductions in FPG were associated with the reduced risk of 10/14 adverse outcomes, with the exceptions being cesarean section, small for gestational age, premature rupture of membranes, and congenital malformation. Reductions in A1C were strongly associated with the reduced risk of cesarean section (<i>r</i> = 0.67, <i>p</i> < 0.001), indicating that the RR (95% confidence interval) for a 1% incremental decrease in A1C was 0.63 (0.49-0.80). <b>Conclusions:</b> Risk reductions in the majority of pregnancy complications in those with diabetes depend on the improvement of GC induced by intensive glucose management.</p>","PeriodicalId":15576,"journal":{"name":"Journal of Diabetes Research","volume":"2025 ","pages":"3490884"},"PeriodicalIF":3.4000,"publicationDate":"2025-06-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12208766/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Diabetes Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/jdr/3490884","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
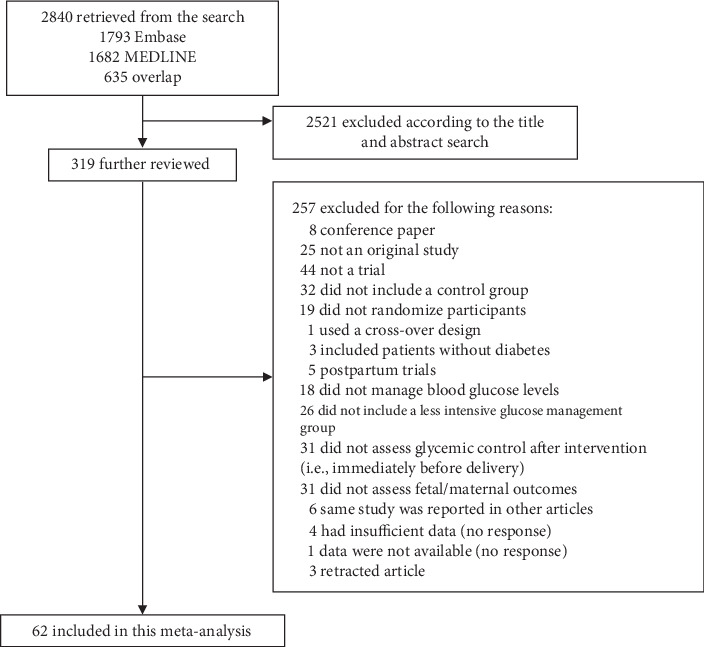
Background: It remains unknown whether improvements in prognosis of pregnancy in patients with diabetes mellitus are dependent on glycemic control (GC). This metaregression analysis was aimed at exploring the relationships between the improvements in GC. Methods: Using Embase and MEDLINE (from Jan. 1, 1950, to Apr. 29, 2024), we searched for randomized controlled trials of intensive glucose management in pregnant women with gestational, pregestational, or overt diabetes mellitus, in which the blood glucose level using any GC indicator and the incidence of any adverse maternal and/or fetal outcome were compared between two groups with different intensities of glucose management. Relative risks (RRs) of individual adverse outcomes were regressed on the reductions in individual GC indicators. Results: We examined the dose-response relationship between reductions in four GC indicators (hemoglobin A1c (A1C), fasting plasma glucose (FPG), 2-h postprandial glucose, and mean blood glucose) and 14 adverse pregnancy outcomes in 62 eligible trials. Reductions in FPG were associated with the reduced risk of 10/14 adverse outcomes, with the exceptions being cesarean section, small for gestational age, premature rupture of membranes, and congenital malformation. Reductions in A1C were strongly associated with the reduced risk of cesarean section (r = 0.67, p < 0.001), indicating that the RR (95% confidence interval) for a 1% incremental decrease in A1C was 0.63 (0.49-0.80). Conclusions: Risk reductions in the majority of pregnancy complications in those with diabetes depend on the improvement of GC induced by intensive glucose management.
期刊介绍:
Journal of Diabetes Research is a peer-reviewed, Open Access journal that publishes research articles, review articles, and clinical studies related to type 1 and type 2 diabetes. The journal welcomes submissions focusing on the epidemiology, etiology, pathogenesis, management, and prevention of diabetes, as well as associated complications, such as diabetic retinopathy, neuropathy and nephropathy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


