Outcomes of Combined Proximal Medial Gastrocnemius Release and Achilles Tendon Debridement and Reinsertion for Calcified Insertional Achilles Tendinopathy.
Daniel Saraiva, Markus Knupp, Daniel Freitas, André Sá Rodrigues, Tiago Pato, José Tulha, Tiago Mota Gomes, Xavier Martín Oliva
{"title":"Outcomes of Combined Proximal Medial Gastrocnemius Release and Achilles Tendon Debridement and Reinsertion for Calcified Insertional Achilles Tendinopathy.","authors":"Daniel Saraiva, Markus Knupp, Daniel Freitas, André Sá Rodrigues, Tiago Pato, José Tulha, Tiago Mota Gomes, Xavier Martín Oliva","doi":"10.1177/24730114251348194","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Gastrocnemius tightness has been implicated in the pathogenesis of calcified insertional Achilles tendinopathy (IAT), Haglund deformity, and Achilles intratendinous calcifications (IC). The aims of this study were to determine long-term clinical and radiographic results of combined proximal medial gastrocnemius release (PMGR) and Achilles tendon debridement and reattachment (ATDR) for patients presenting with symptomatic calcified IAT.</p><p><strong>Methods: </strong>A retrospective cohort study was performed in order to determine clinical and radiographic outcomes of PMGR and ATDR for patients presenting with symptomatic calcified IAT, at a minimum follow-up of 30 months. Patient satisfaction was assessed at last available follow-up as very satisfied, satisfied, and unsatisfied. Clinical assessment was performed evaluating preoperative and last available follow-up visual analog scale for pain (VAS-P) and the Foot and Ankle Outcome Score (FAOS). Radiographic evaluation included Fowler-Phillip angle, calcification length, calcification width, and presence of Achilles IC, measured on standard weightbearing lateral calibrated radiograph of the foot preoperatively and last available follow-up evaluation for each patient.</p><p><strong>Results: </strong>The mean follow-up was 46 (range, 30-72) months. We registered 45 \"very satisfied\" patients (84.91%), 6 \"satisfied\" patients (11.32%), and 2 \"unsatisfied\" patients (3.77%), as well as statistically significant improvement on both clinical scores tested. We found statistically significant differences between the initial evaluation and last available follow-up on all radiographic measurements. There was no significant radiographic recurrence of calcified IAT, whereas minor Achilles intratendinous calcifications were found in 10 patients (18.87%).</p><p><strong>Conclusion: </strong>Combined PMGR and ATDR provides significant clinical and radiographic improvement for patients presenting with symptomatic calcified IAT and, although not preventing radiographic recurrence of minor Achilles IC, may reduce the rate of radiographic recurrence of calcified IAT, though the lack of a control group limits causal inference.</p><p><strong>Level of evidence: </strong>Level III, retrospective cohort study.</p>","PeriodicalId":12429,"journal":{"name":"Foot & Ankle Orthopaedics","volume":"10 2","pages":"24730114251348194"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12202936/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Foot & Ankle Orthopaedics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/24730114251348194","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Gastrocnemius tightness has been implicated in the pathogenesis of calcified insertional Achilles tendinopathy (IAT), Haglund deformity, and Achilles intratendinous calcifications (IC). The aims of this study were to determine long-term clinical and radiographic results of combined proximal medial gastrocnemius release (PMGR) and Achilles tendon debridement and reattachment (ATDR) for patients presenting with symptomatic calcified IAT.
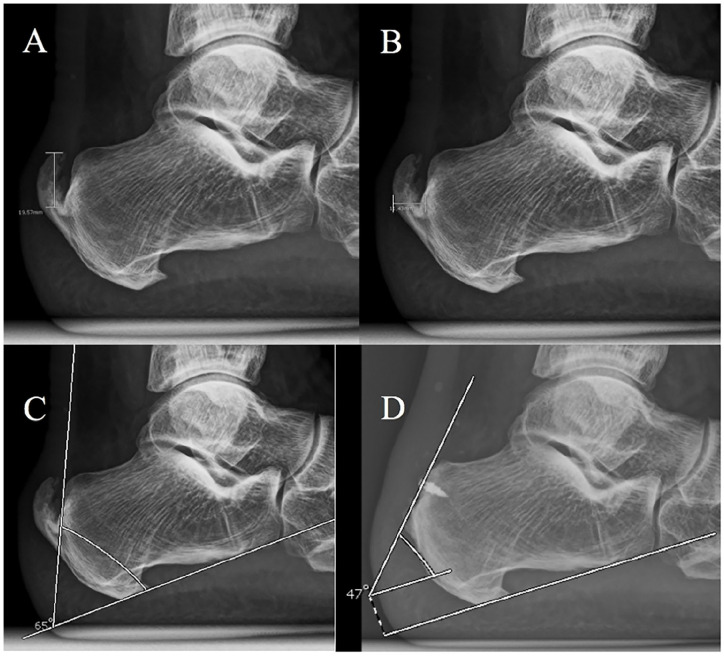
Methods: A retrospective cohort study was performed in order to determine clinical and radiographic outcomes of PMGR and ATDR for patients presenting with symptomatic calcified IAT, at a minimum follow-up of 30 months. Patient satisfaction was assessed at last available follow-up as very satisfied, satisfied, and unsatisfied. Clinical assessment was performed evaluating preoperative and last available follow-up visual analog scale for pain (VAS-P) and the Foot and Ankle Outcome Score (FAOS). Radiographic evaluation included Fowler-Phillip angle, calcification length, calcification width, and presence of Achilles IC, measured on standard weightbearing lateral calibrated radiograph of the foot preoperatively and last available follow-up evaluation for each patient.
Results: The mean follow-up was 46 (range, 30-72) months. We registered 45 "very satisfied" patients (84.91%), 6 "satisfied" patients (11.32%), and 2 "unsatisfied" patients (3.77%), as well as statistically significant improvement on both clinical scores tested. We found statistically significant differences between the initial evaluation and last available follow-up on all radiographic measurements. There was no significant radiographic recurrence of calcified IAT, whereas minor Achilles intratendinous calcifications were found in 10 patients (18.87%).
Conclusion: Combined PMGR and ATDR provides significant clinical and radiographic improvement for patients presenting with symptomatic calcified IAT and, although not preventing radiographic recurrence of minor Achilles IC, may reduce the rate of radiographic recurrence of calcified IAT, though the lack of a control group limits causal inference.
Level of evidence: Level III, retrospective cohort study.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


