Acute Lymphoblastic Leukemia Presenting With Initial Hyperbilirubinemia and Significantly Elevated Liver Transaminases: A Rare Pediatric Case With Unadjusted Chemotherapy.
Atbin Latifi, Mahbod Soltani, Mohammad Satarzadeh, Negar Pourahmadian, Amirreza Hesami Rad
{"title":"Acute Lymphoblastic Leukemia Presenting With Initial Hyperbilirubinemia and Significantly Elevated Liver Transaminases: A Rare Pediatric Case With Unadjusted Chemotherapy.","authors":"Atbin Latifi, Mahbod Soltani, Mohammad Satarzadeh, Negar Pourahmadian, Amirreza Hesami Rad","doi":"10.1177/11795476251351514","DOIUrl":null,"url":null,"abstract":"<p><p>Acute lymphoblastic leukemia (ALL) rarely presents with initial liver failure. We describe a 9-year-old boy with no past medical history who presented with jaundice, hyperbilirubinemia (total bilirubin 13.1 mg/dL), and significantly elevated transaminases (ALT 1283 U/L, AST 1325 U/L). Bone marrow aspiration confirmed precursor B-cell ALL. Despite severe hepatic dysfunction, full-dose induction chemotherapy was administered following corticosteroid therapy, leading to rapid improvement in liver function and normalization by day 29. No complications were observed, and at the end of induction, minimal residual disease was 0.001%. This case of successful unadjusted chemotherapy, with leukemic infiltration identified as the etiology of hepatitis, underscores the importance of early diagnosis, multidisciplinary management, close monitoring, and highlights the need for further investigation into safe treatment protocols in such cases.</p>","PeriodicalId":10357,"journal":{"name":"Clinical Medicine Insights. Case Reports","volume":"18 ","pages":"11795476251351514"},"PeriodicalIF":0.6000,"publicationDate":"2025-06-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12202906/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795476251351514","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
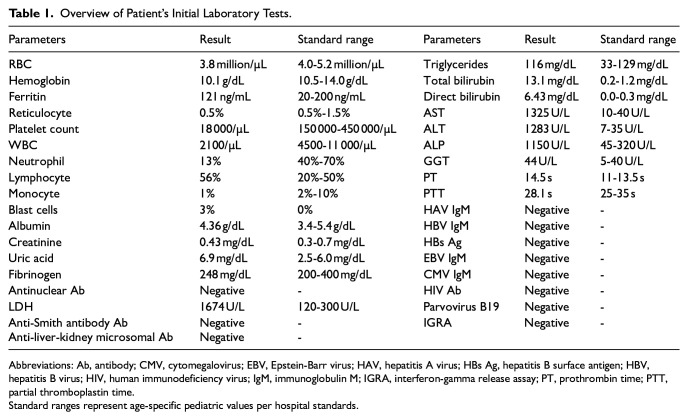
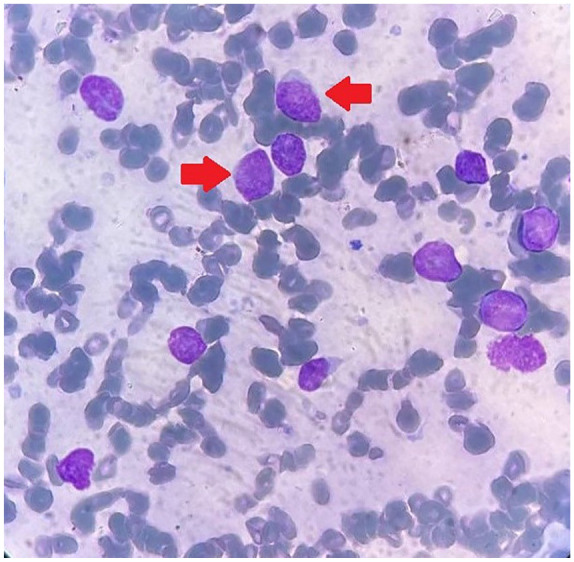
Acute lymphoblastic leukemia (ALL) rarely presents with initial liver failure. We describe a 9-year-old boy with no past medical history who presented with jaundice, hyperbilirubinemia (total bilirubin 13.1 mg/dL), and significantly elevated transaminases (ALT 1283 U/L, AST 1325 U/L). Bone marrow aspiration confirmed precursor B-cell ALL. Despite severe hepatic dysfunction, full-dose induction chemotherapy was administered following corticosteroid therapy, leading to rapid improvement in liver function and normalization by day 29. No complications were observed, and at the end of induction, minimal residual disease was 0.001%. This case of successful unadjusted chemotherapy, with leukemic infiltration identified as the etiology of hepatitis, underscores the importance of early diagnosis, multidisciplinary management, close monitoring, and highlights the need for further investigation into safe treatment protocols in such cases.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


