One-year survival after critical care as a decision basis for advance care directives in general medicine: Real word data analysis of 149,144 patients.
Constantin Unger, Felix Werner, Bettina Engel, Thomas Kühlein, Christoph Schulz, Christian Kümpel, Johannes Gorkotte, Susann Hueber
{"title":"One-year survival after critical care as a decision basis for advance care directives in general medicine: Real word data analysis of 149,144 patients.","authors":"Constantin Unger, Felix Werner, Bettina Engel, Thomas Kühlein, Christoph Schulz, Christian Kümpel, Johannes Gorkotte, Susann Hueber","doi":"10.1371/journal.pone.0326031","DOIUrl":null,"url":null,"abstract":"<p><p>Providing counsel on advance care directives is challenging for general practitioners. Counselling is done on unknown future circumstances of possible critical illness and critical care in intensive care units. Following the principles of evidence-based medicine, the physician's task is to communicate evidence and elucidate the patient's position on it. However, suitable evidence of chances of survival in case of critical illness is lacking. Aim of this study was to generate long-term survival rates of patients receiving critical care as evidence for general practitioners who provide counselling for patients on advance care directives. We conducted a retrospective cohort study analysing one-year survival rates of critical care using German health insurance claims data from an anonymised nationwide health claims data pool of over five million German patients. All patients over 18 years of age receiving critical care for the first time were included.Main outcome of our study were one-year survival probabilities depending on age and on acute life prolonging procedures. Procedures analysed were non-invasive and invasive mechanical ventilation (nMV, iMV), renal replacement therapy (RRT), their combinations (nMV + RRT, iMV + RRT), and cardiopulmonary resuscitation (CPR). A total of 149,144 datasets was analysed. One-year survival probability of all patients was 77.5%. Survival rates ranged from 94.5% in patients under 50 without any further acute life prolonging procedures to 16.4% in those older than 80 who received iMV + RRT. The application of at least one procedure was associated with an increased risk of death (HR 3.06, 95% CI 2.99 to 3.12) as was CPR (HR 4.22, 95% CI 4.07 to 4.37). Differences between pre- and COVID periods were modest. To enable patient's decision-making in creating advance care directives, our results provide easily applicable external evidence for general practitioners counselling on advance care directives by providing probabilities of survival in critical care.</p>","PeriodicalId":20189,"journal":{"name":"PLoS ONE","volume":"20 6","pages":"e0326031"},"PeriodicalIF":2.6000,"publicationDate":"2025-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12204473/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS ONE","FirstCategoryId":"103","ListUrlMain":"https://doi.org/10.1371/journal.pone.0326031","RegionNum":3,"RegionCategory":"综合性期刊","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MULTIDISCIPLINARY SCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
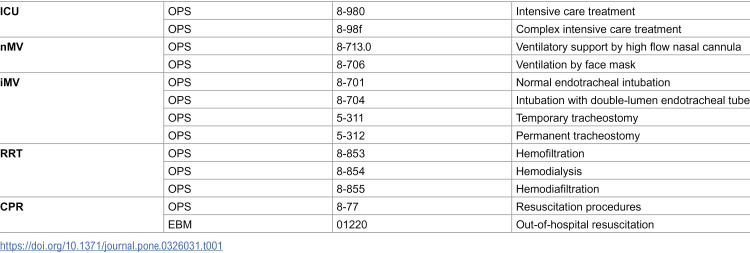
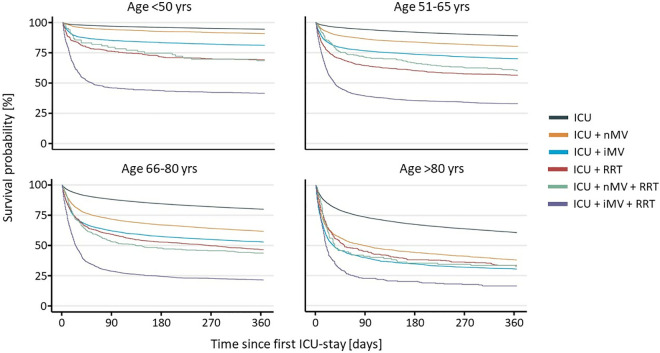
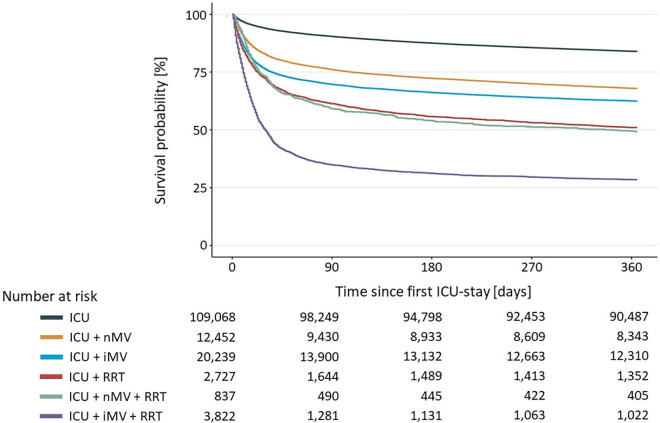
Providing counsel on advance care directives is challenging for general practitioners. Counselling is done on unknown future circumstances of possible critical illness and critical care in intensive care units. Following the principles of evidence-based medicine, the physician's task is to communicate evidence and elucidate the patient's position on it. However, suitable evidence of chances of survival in case of critical illness is lacking. Aim of this study was to generate long-term survival rates of patients receiving critical care as evidence for general practitioners who provide counselling for patients on advance care directives. We conducted a retrospective cohort study analysing one-year survival rates of critical care using German health insurance claims data from an anonymised nationwide health claims data pool of over five million German patients. All patients over 18 years of age receiving critical care for the first time were included.Main outcome of our study were one-year survival probabilities depending on age and on acute life prolonging procedures. Procedures analysed were non-invasive and invasive mechanical ventilation (nMV, iMV), renal replacement therapy (RRT), their combinations (nMV + RRT, iMV + RRT), and cardiopulmonary resuscitation (CPR). A total of 149,144 datasets was analysed. One-year survival probability of all patients was 77.5%. Survival rates ranged from 94.5% in patients under 50 without any further acute life prolonging procedures to 16.4% in those older than 80 who received iMV + RRT. The application of at least one procedure was associated with an increased risk of death (HR 3.06, 95% CI 2.99 to 3.12) as was CPR (HR 4.22, 95% CI 4.07 to 4.37). Differences between pre- and COVID periods were modest. To enable patient's decision-making in creating advance care directives, our results provide easily applicable external evidence for general practitioners counselling on advance care directives by providing probabilities of survival in critical care.
期刊介绍:
PLOS ONE is an international, peer-reviewed, open-access, online publication. PLOS ONE welcomes reports on primary research from any scientific discipline. It provides:
* Open-access—freely accessible online, authors retain copyright
* Fast publication times
* Peer review by expert, practicing researchers
* Post-publication tools to indicate quality and impact
* Community-based dialogue on articles
* Worldwide media coverage

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


