{"title":"Outcomes of Older Patients Undergoing Surgery for Esophageal Squamous Cell Carcinoma.","authors":"Takuya Iguchi, Satoshi Nakamura, Masato Kitazawa, Yuta Yamamoto, Satoru Miyazaki, Nao Hondo, Masahiro Kataoka, Hirokazu Tanaka, Ryosuke Aoki, Park Yonghan, Yuji Soejima","doi":"10.21873/invivo.14024","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/aim: </strong>Esophageal cancer is a leading cause of death among males worldwide, including Japan, where squamous cell carcinoma is the most common type. Treatment decisions can be complicated, especially for older patients undergoing esophagectomy, which, while effective, is invasive and incurs significant risks.</p><p><strong>Patients and methods: </strong>A retrospective review of 126 consecutive patients with esophageal squamous cell carcinoma (ESCC) who underwent open or thoracoscopic esophagectomy between January 2010 and April 2023 was conducted. Older patients aged ≥75 years (n=24) were compared with non-older patients aged <75 years (n=102).</p><p><strong>Results: </strong>Both estimated Glomerular Filtration Rate (eGFR) and albumin levels were notably lower in older patients with a more extensive medical history and higher American Society of Anesthesiologists Physical Status scores. However, there were no differences in sex, Body Mass Index, or pathological stage. Both groups showed similar characteristics in terms of the esophagectomy approach, field dissection, preoperative treatment, operation duration, bleeding, postoperative complications, and hospital stay. No differences were observed between non-older and older groups regarding overall survival (OS), recurrence-free survival (RFS), and disease-specific survival (DSS) (5-year OS: 63.4% <i>vs</i>. 29.2%, respectively, <i>p</i>=0.119; 5-year RFS: 48.6% <i>vs</i>. 33.9%, respectively, <i>p</i>=0.612; 5-year DSS: 73.2% and 46.2%, respectively, <i>p</i>=0.978). Additionally, multivariate survival analysis indicated that pathological N stage [hazard ratio (HR)=2.13; 95% confidence interval (CI)=1.10-4.12; <i>p</i>=0.025] and pathological T stage (HR=2.16; 95%CI=1.13-4.15; <i>p</i>=0.021) were independent prognostic factors for OS. However, age was not a prognostic factor.</p><p><strong>Conclusion: </strong>Esophagectomy for patients aged 75 years or older provides comparable long-term outcomes without increasing postoperative complications compared with patients younger than 75 years.</p>","PeriodicalId":13364,"journal":{"name":"In vivo","volume":"39 4","pages":"2286-2294"},"PeriodicalIF":1.8000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12223664/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"In vivo","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21873/invivo.14024","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background/aim: Esophageal cancer is a leading cause of death among males worldwide, including Japan, where squamous cell carcinoma is the most common type. Treatment decisions can be complicated, especially for older patients undergoing esophagectomy, which, while effective, is invasive and incurs significant risks.
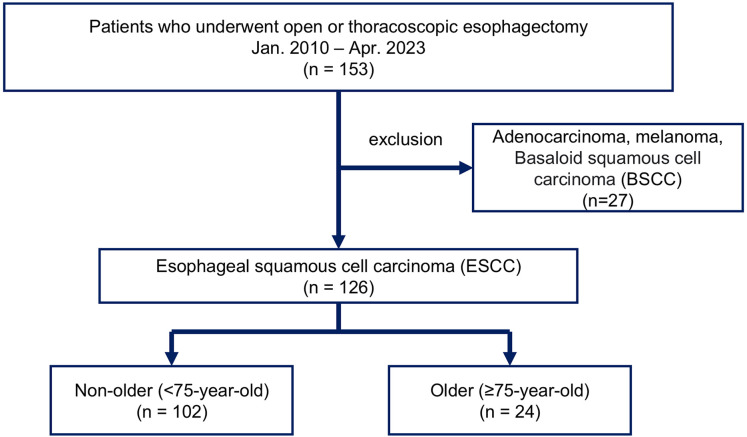
Patients and methods: A retrospective review of 126 consecutive patients with esophageal squamous cell carcinoma (ESCC) who underwent open or thoracoscopic esophagectomy between January 2010 and April 2023 was conducted. Older patients aged ≥75 years (n=24) were compared with non-older patients aged <75 years (n=102).
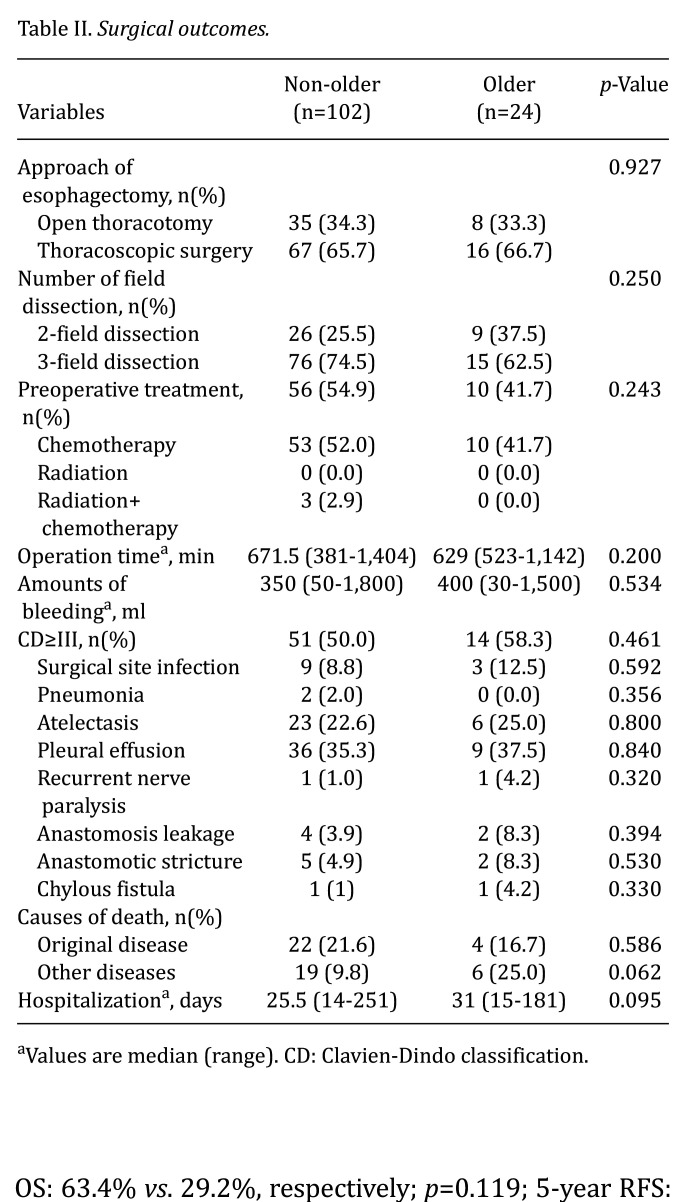
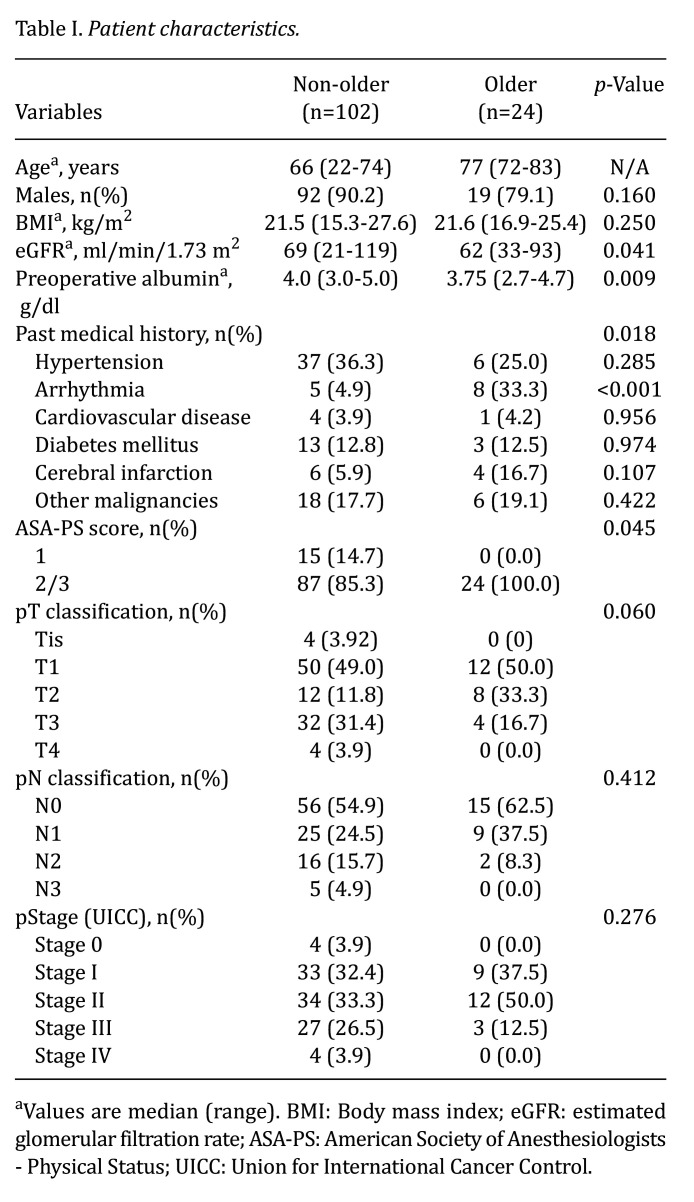
Results: Both estimated Glomerular Filtration Rate (eGFR) and albumin levels were notably lower in older patients with a more extensive medical history and higher American Society of Anesthesiologists Physical Status scores. However, there were no differences in sex, Body Mass Index, or pathological stage. Both groups showed similar characteristics in terms of the esophagectomy approach, field dissection, preoperative treatment, operation duration, bleeding, postoperative complications, and hospital stay. No differences were observed between non-older and older groups regarding overall survival (OS), recurrence-free survival (RFS), and disease-specific survival (DSS) (5-year OS: 63.4% vs. 29.2%, respectively, p=0.119; 5-year RFS: 48.6% vs. 33.9%, respectively, p=0.612; 5-year DSS: 73.2% and 46.2%, respectively, p=0.978). Additionally, multivariate survival analysis indicated that pathological N stage [hazard ratio (HR)=2.13; 95% confidence interval (CI)=1.10-4.12; p=0.025] and pathological T stage (HR=2.16; 95%CI=1.13-4.15; p=0.021) were independent prognostic factors for OS. However, age was not a prognostic factor.
Conclusion: Esophagectomy for patients aged 75 years or older provides comparable long-term outcomes without increasing postoperative complications compared with patients younger than 75 years.
背景/目的:食管癌是世界范围内男性死亡的主要原因,包括日本,其中鳞状细胞癌是最常见的类型。治疗决策可能很复杂,特别是对于接受食管切除术的老年患者,虽然有效,但具有侵入性,并且会产生重大风险。患者和方法:回顾性分析了2010年1月至2023年4月期间连续126例食管鳞状细胞癌(ESCC)接受开放或胸腔镜食管切除术的患者。年龄≥75岁的老年患者(n=24)与年龄较大的非老年患者进行比较结果:在病史更广泛且美国麻醉医师协会身体状况评分较高的老年患者中,肾小球滤过率(eGFR)和白蛋白水平的估计值均明显较低。然而,在性别、身体质量指数和病理分期方面没有差异。两组在食管切除术入路、野区清扫、术前处理、手术时间、出血、术后并发症、住院时间等方面均表现出相似的特点。非老年组和老年组在总生存率(OS)、无复发生存率(RFS)和疾病特异性生存率(DSS)方面均无差异(5年生存率分别为63.4% vs 29.2%, p=0.119;5年RFS分别为48.6% vs. 33.9%, p=0.612;5年DSS分别为73.2%和46.2%,p=0.978)。此外,多变量生存分析显示病理N期[危险比(HR)=2.13;95%置信区间(CI)=1.10-4.12;p=0.025]病理T分期(HR=2.16;95%可信区间= 1.13 - -4.15;p=0.021)是OS的独立预后因素。然而,年龄不是预后因素。结论:与75岁以下患者相比,75岁及以上患者行食管切除术可提供相当的长期预后,且不会增加术后并发症。
期刊介绍:
IN VIVO is an international peer-reviewed journal designed to bring together original high quality works and reviews on experimental and clinical biomedical research within the frames of physiology, pathology and disease management.
The topics of IN VIVO include: 1. Experimental development and application of new diagnostic and therapeutic procedures; 2. Pharmacological and toxicological evaluation of new drugs, drug combinations and drug delivery systems; 3. Clinical trials; 4. Development and characterization of models of biomedical research; 5. Cancer diagnosis and treatment; 6. Immunotherapy and vaccines; 7. Radiotherapy, Imaging; 8. Tissue engineering, Regenerative medicine; 9. Carcinogenesis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


