Ganbin Li, Xiao Zhang, Xiaoyuan Qiu, Lai Xu, Junyang Lu, Bin Wu, Yi Xiao, Guole Lin
{"title":"Clinical characteristics and survival outcomes of rectal cancer patients across different mrT3 substages determined by rectal MRI.","authors":"Ganbin Li, Xiao Zhang, Xiaoyuan Qiu, Lai Xu, Junyang Lu, Bin Wu, Yi Xiao, Guole Lin","doi":"10.1007/s00384-025-04935-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Locally advanced rectal cancer (LARC) staged as mrT3 could be further subdivided into mrT3a to T3d based on depth of tumor invasion through the muscularis propria. Limited evidence exists to compare the differences across subgroups.</p><p><strong>Methods: </strong>Clinical data from patients between January 2018 and 2022 were collected. The study included patients with mrT3 LARC who received neoadjuvant chemoradiotherapy (NCRT). Based on depth of invasion through muscularis propria, patients were categorized into three groups: mrT3a (< 5 mm), mrT3b (5~10 mm), mrT3c~d group (> 10 mm). The outcomes were disease-free survival (DFS), pathological complete response (pCR), tumor recurrence and metastasis.</p><p><strong>Results: </strong>A total of 295 patients were identified, including 65 (22.0%) in mrT3a, 155 (52.5%) in mrT3b, and 75 (25.5%) in mrT3c~d group. The tumor vertical diameter was larger in mrT3c/d group (46.3 ± 13.7 mm), compared to mrT3a (39.4 ± 14.3 mm) and mrT3b (39.8 ± 12.1 mm) groups (P < 0.001). The positive rates of mesorectal fascia (61.3% vs. 30.3% vs. 7.7%, P < 0.001) and extramural vascular invasion (62.7% vs. 40.0% vs. 27.7%, P < 0.001) were significantly higher in mrT3c/d group compared to mrT3a and mrT3b groups. The estimated pCR rates were 33.9% for mrT3a, 32.3% for mrT3b, and 21.3% for mrT3c/d group (P = 0.172). The median follow-up time was 43 (29-58) months. The metastasis and local recurrence rates were 8.8% and 2.4%. The 3y-DFS rates were 92.2% for mrT3a, 87.7% for mrT3b, and 86.2% for mrT3c/d (P = 0.549).</p><p><strong>Conclusion: </strong>Despite mrT3c/d patients presenting with more aggressive baseline features, standardized NCRT followed by radical surgery effectively mitigated survival disparities across mrT3 substages. These findings suggest that mrT3 subclassification may not independently predict long-term survival outcomes when patients receive optimal multimodal therapy.</p>","PeriodicalId":13789,"journal":{"name":"International Journal of Colorectal Disease","volume":"40 1","pages":"147"},"PeriodicalIF":2.3000,"publicationDate":"2025-06-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12204897/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Colorectal Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00384-025-04935-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Locally advanced rectal cancer (LARC) staged as mrT3 could be further subdivided into mrT3a to T3d based on depth of tumor invasion through the muscularis propria. Limited evidence exists to compare the differences across subgroups.
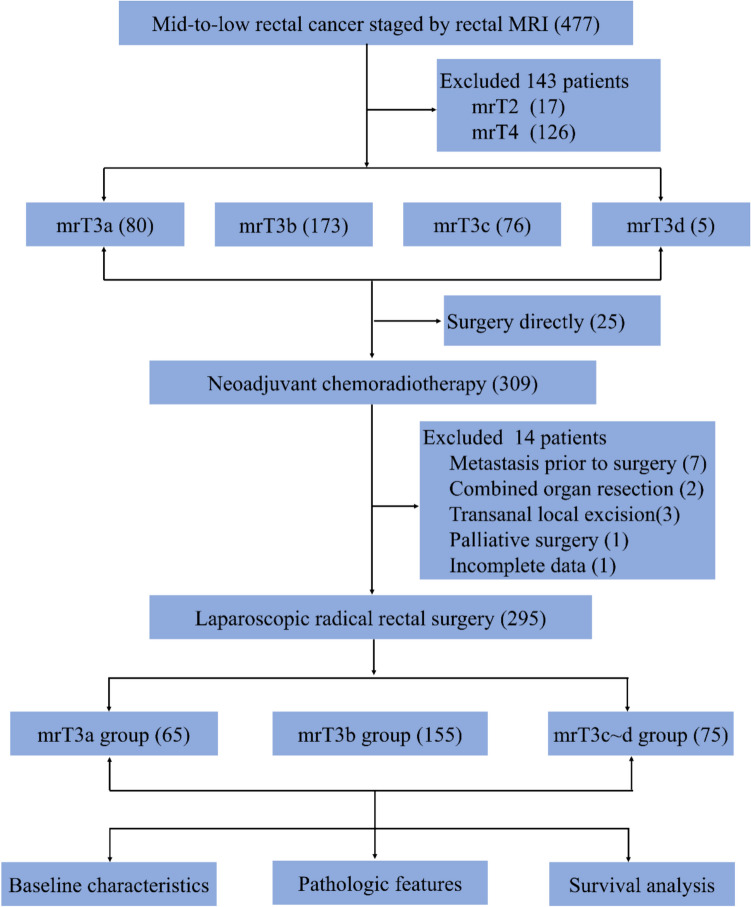
Methods: Clinical data from patients between January 2018 and 2022 were collected. The study included patients with mrT3 LARC who received neoadjuvant chemoradiotherapy (NCRT). Based on depth of invasion through muscularis propria, patients were categorized into three groups: mrT3a (< 5 mm), mrT3b (5~10 mm), mrT3c~d group (> 10 mm). The outcomes were disease-free survival (DFS), pathological complete response (pCR), tumor recurrence and metastasis.
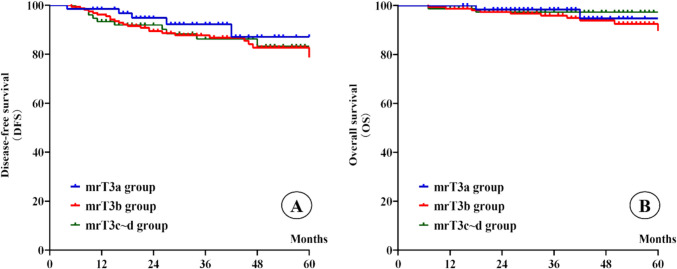
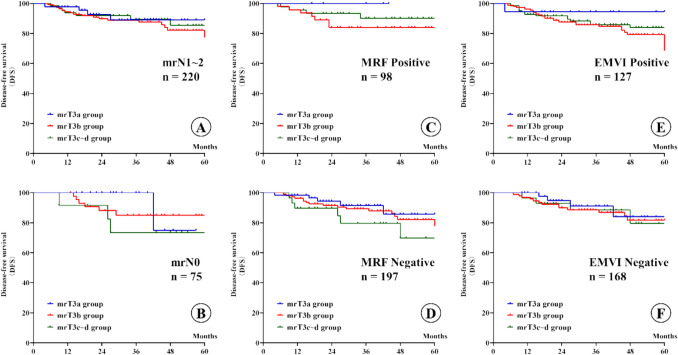
Results: A total of 295 patients were identified, including 65 (22.0%) in mrT3a, 155 (52.5%) in mrT3b, and 75 (25.5%) in mrT3c~d group. The tumor vertical diameter was larger in mrT3c/d group (46.3 ± 13.7 mm), compared to mrT3a (39.4 ± 14.3 mm) and mrT3b (39.8 ± 12.1 mm) groups (P < 0.001). The positive rates of mesorectal fascia (61.3% vs. 30.3% vs. 7.7%, P < 0.001) and extramural vascular invasion (62.7% vs. 40.0% vs. 27.7%, P < 0.001) were significantly higher in mrT3c/d group compared to mrT3a and mrT3b groups. The estimated pCR rates were 33.9% for mrT3a, 32.3% for mrT3b, and 21.3% for mrT3c/d group (P = 0.172). The median follow-up time was 43 (29-58) months. The metastasis and local recurrence rates were 8.8% and 2.4%. The 3y-DFS rates were 92.2% for mrT3a, 87.7% for mrT3b, and 86.2% for mrT3c/d (P = 0.549).
Conclusion: Despite mrT3c/d patients presenting with more aggressive baseline features, standardized NCRT followed by radical surgery effectively mitigated survival disparities across mrT3 substages. These findings suggest that mrT3 subclassification may not independently predict long-term survival outcomes when patients receive optimal multimodal therapy.
期刊介绍:
The International Journal of Colorectal Disease, Clinical and Molecular Gastroenterology and Surgery aims to publish novel and state-of-the-art papers which deal with the physiology and pathophysiology of diseases involving the entire gastrointestinal tract. In addition to original research articles, the following categories will be included: reviews (usually commissioned but may also be submitted), case reports, letters to the editor, and protocols on clinical studies.
The journal offers its readers an interdisciplinary forum for clinical science and molecular research related to gastrointestinal disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


