{"title":"Impact of Adjuvant Chemotherapy Following Neoadjuvant Concurrent Chemoradiotherapy and Total Mesorectal Excision in Rectal Cancer.","authors":"Yu-Shih Liu, Jen-Kou Lin, Tzu-Chen Lin, Wei-Shone Chen, Shung-Haur Yang, Huann-Shenn Wang, Shih-Ching Chang, Yuan-Tzu Lan, Chun-Chi Lin, Hung-Hsin Lin, Jeng-Kai Jiang","doi":"10.21873/invivo.14027","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/aim: </strong>This study investigated the efficacy of adjuvant chemotherapy (ACT) after total mesorectal excision (TME) for rectal cancer in patients who responded well to neoadjuvant concurrent chemoradiotherapy (nCCRT).</p><p><strong>Patients and methods: </strong>This retrospective study included patients with rectal cancer treated at Taipei Veterans General Hospital (2009-2017). Among 302 patients who underwent nCCRT and TME, 178 good responders [pathologic complete response (pCR), pT1, or pT2] were analyzed. Patients were grouped based on ACT administration. Primary outcomes included disease-free survival (DFS) and recurrence. Kaplan-Meier survival analysis and Cox proportional hazards regression were used to assess ACT efficacy.</p><p><strong>Results: </strong>The ACT group (n=96) had poorer baseline disease characteristics, including higher initial clinical T and N stages. However, recurrence rates did not differ significantly between ACT and non-ACT groups (23.2% <i>vs</i>. 17.7%, <i>p</i>=0.271). DFS curves showed no significant difference between ACT and non-ACT groups (<i>p</i>=0.360). Multivariable analysis confirmed that ACT was not significantly associated with DFS [adjusted hazard ratio (aHR)=0.76, 95% confidence interval (CI)=0.37-1.59]. However, the advanced surgical pT stage (pT3-pT4) was an independent predictor of recurrence (aHR=3.24, 95%CI=1.01-10.38, <i>p</i>=0.047).</p><p><strong>Conclusion: </strong>The role of ACT remains inconclusive after TME for rectal cancer in patients who respond well to nCCRT. Surgical pT stage, particularly pT3 and pT4, remain a significant predictor of recurrence, emphasizing its importance in risk stratification.</p>","PeriodicalId":13364,"journal":{"name":"In vivo","volume":"39 4","pages":"2311-2319"},"PeriodicalIF":1.8000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12223617/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"In vivo","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21873/invivo.14027","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background/aim: This study investigated the efficacy of adjuvant chemotherapy (ACT) after total mesorectal excision (TME) for rectal cancer in patients who responded well to neoadjuvant concurrent chemoradiotherapy (nCCRT).
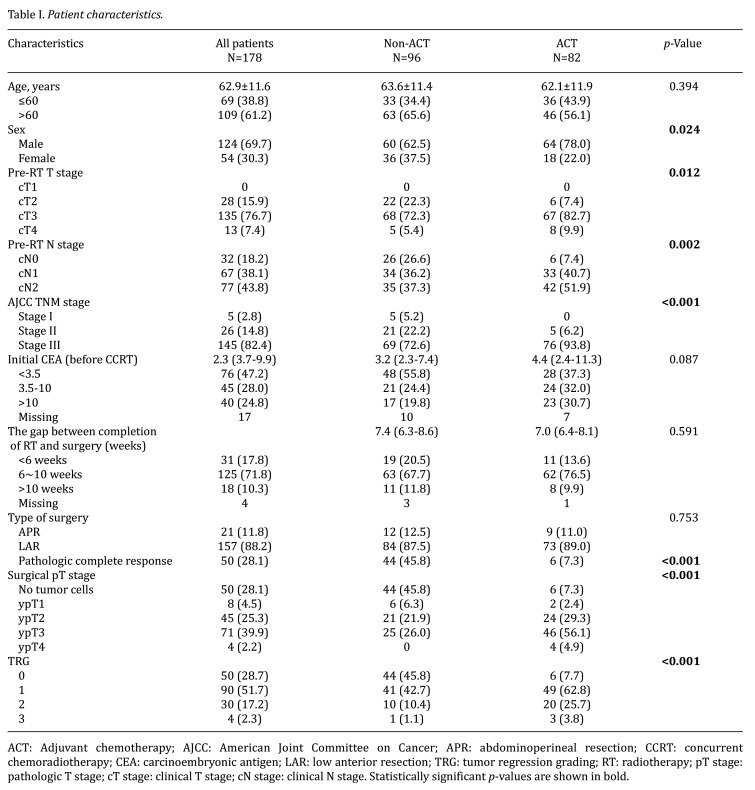
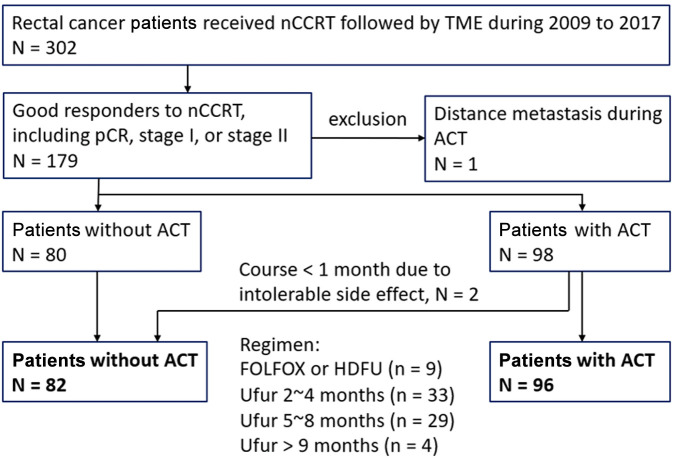
Patients and methods: This retrospective study included patients with rectal cancer treated at Taipei Veterans General Hospital (2009-2017). Among 302 patients who underwent nCCRT and TME, 178 good responders [pathologic complete response (pCR), pT1, or pT2] were analyzed. Patients were grouped based on ACT administration. Primary outcomes included disease-free survival (DFS) and recurrence. Kaplan-Meier survival analysis and Cox proportional hazards regression were used to assess ACT efficacy.
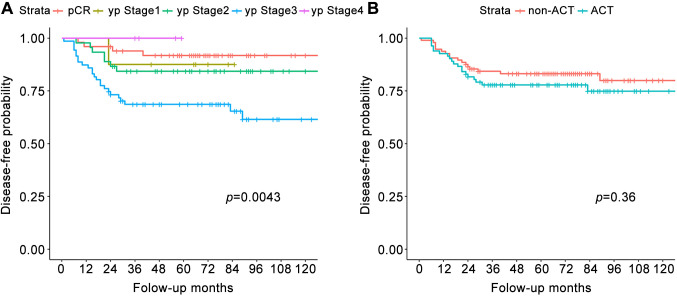
Results: The ACT group (n=96) had poorer baseline disease characteristics, including higher initial clinical T and N stages. However, recurrence rates did not differ significantly between ACT and non-ACT groups (23.2% vs. 17.7%, p=0.271). DFS curves showed no significant difference between ACT and non-ACT groups (p=0.360). Multivariable analysis confirmed that ACT was not significantly associated with DFS [adjusted hazard ratio (aHR)=0.76, 95% confidence interval (CI)=0.37-1.59]. However, the advanced surgical pT stage (pT3-pT4) was an independent predictor of recurrence (aHR=3.24, 95%CI=1.01-10.38, p=0.047).
Conclusion: The role of ACT remains inconclusive after TME for rectal cancer in patients who respond well to nCCRT. Surgical pT stage, particularly pT3 and pT4, remain a significant predictor of recurrence, emphasizing its importance in risk stratification.
期刊介绍:
IN VIVO is an international peer-reviewed journal designed to bring together original high quality works and reviews on experimental and clinical biomedical research within the frames of physiology, pathology and disease management.
The topics of IN VIVO include: 1. Experimental development and application of new diagnostic and therapeutic procedures; 2. Pharmacological and toxicological evaluation of new drugs, drug combinations and drug delivery systems; 3. Clinical trials; 4. Development and characterization of models of biomedical research; 5. Cancer diagnosis and treatment; 6. Immunotherapy and vaccines; 7. Radiotherapy, Imaging; 8. Tissue engineering, Regenerative medicine; 9. Carcinogenesis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


