David Xiao, Yency Forero, Michael N Kammer, Heidi Chen, Rafael Paez, Brent E Heideman, Oreoluwa Owoseeni, Ian Johnson, Stephen A Deppen, Eric L Grogan, Fabien Maldonado
{"title":"Radiomic 'Stress Test': exploration of a deep learning radiomic model in a high-risk prospective lung nodule cohort.","authors":"David Xiao, Yency Forero, Michael N Kammer, Heidi Chen, Rafael Paez, Brent E Heideman, Oreoluwa Owoseeni, Ian Johnson, Stephen A Deppen, Eric L Grogan, Fabien Maldonado","doi":"10.1136/bmjresp-2024-002687","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Indeterminate pulmonary nodules (IPNs) are commonly biopsied to ascertain a diagnosis of lung cancer, but many are ultimately benign. The Lung Cancer Prediction (LCP) score is a commercially available deep learning radiomic model with strong diagnostic performance in incidentally identified IPNs, but its potential use to reduce the need for invasive procedures has not been evaluated in patients with nodules for which a biopsy has been recommended.</p><p><strong>Methods: </strong>In this prospectively collected, retrospective blinded evaluation, the probability of cancer in consecutively biopsied IPNs at a tertiary care centre was calculated using the Mayo Clinic prediction model and categorised into low, intermediate and high-probability groups by applying <10% no-test and >70% treatment thresholds per British Thoracic Society guidelines. We evaluated the diagnostic performance of the Mayo Clinic model, the LCP radiomic model and an integrated model combining the LCP score with statistically selected clinical variables (age, spiculation and upper lobe location) using stepwise logistic regression. Performance was assessed using area under the receiver operating characteristic curve (AUC), F1 score and reclassification analysis based on the bias-corrected clinical net reclassification index.</p><p><strong>Results: </strong>The study population included 196 malignant and 125 benign IPNs (61% prevalence of malignancy). The Mayo Clinic model's AUC was 0.69 (0.63-0.75), LCP's AUC was 0.67 (0.61-0.73) and the integrated model combining LCP with statistically selected clinical variables (age, spiculation and upper lobe location) had the highest AUC of 0.75 (0.69-0.80). The integrated model demonstrated improved classification, with an F1 score of 0.645 (0.572-0.716) and a significantly higher AUC compared with the Mayo Clinic model (p=0.046). Reclassification analysis showed a clinical net reclassification index of 0.36 (0.21-0.53) for benign IPNs with eight correctly downgraded intermediate-risk benign nodules and no malignant nodules misclassified into the low-risk category.</p><p><strong>Conclusion: </strong>Incorporating LCP with select clinical variables results in an improvement in malignancy risk prediction and nodule classification and could reduce unnecessary invasive biopsies for IPNs.</p>","PeriodicalId":9048,"journal":{"name":"BMJ Open Respiratory Research","volume":"12 1","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2025-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12207176/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Respiratory Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjresp-2024-002687","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Indeterminate pulmonary nodules (IPNs) are commonly biopsied to ascertain a diagnosis of lung cancer, but many are ultimately benign. The Lung Cancer Prediction (LCP) score is a commercially available deep learning radiomic model with strong diagnostic performance in incidentally identified IPNs, but its potential use to reduce the need for invasive procedures has not been evaluated in patients with nodules for which a biopsy has been recommended.
Methods: In this prospectively collected, retrospective blinded evaluation, the probability of cancer in consecutively biopsied IPNs at a tertiary care centre was calculated using the Mayo Clinic prediction model and categorised into low, intermediate and high-probability groups by applying <10% no-test and >70% treatment thresholds per British Thoracic Society guidelines. We evaluated the diagnostic performance of the Mayo Clinic model, the LCP radiomic model and an integrated model combining the LCP score with statistically selected clinical variables (age, spiculation and upper lobe location) using stepwise logistic regression. Performance was assessed using area under the receiver operating characteristic curve (AUC), F1 score and reclassification analysis based on the bias-corrected clinical net reclassification index.
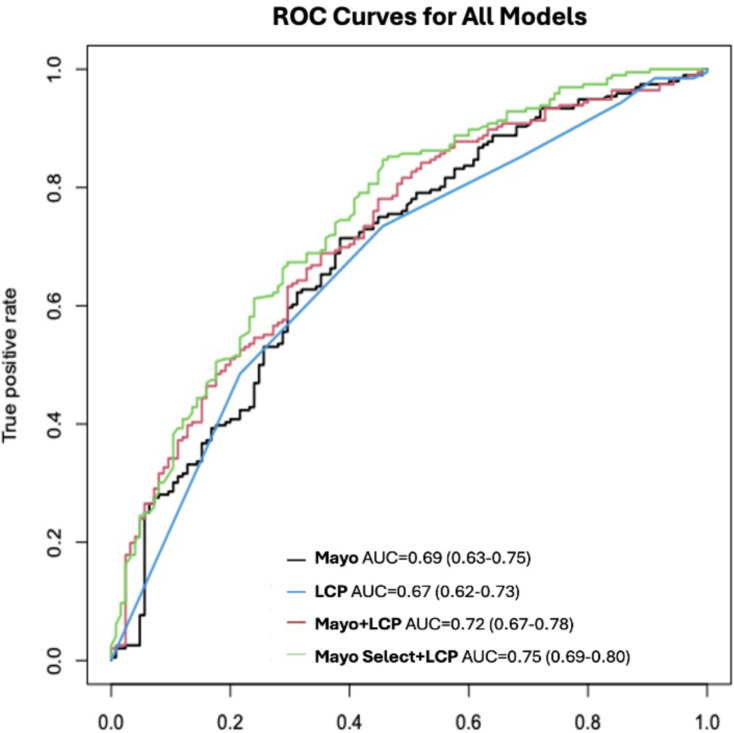
Results: The study population included 196 malignant and 125 benign IPNs (61% prevalence of malignancy). The Mayo Clinic model's AUC was 0.69 (0.63-0.75), LCP's AUC was 0.67 (0.61-0.73) and the integrated model combining LCP with statistically selected clinical variables (age, spiculation and upper lobe location) had the highest AUC of 0.75 (0.69-0.80). The integrated model demonstrated improved classification, with an F1 score of 0.645 (0.572-0.716) and a significantly higher AUC compared with the Mayo Clinic model (p=0.046). Reclassification analysis showed a clinical net reclassification index of 0.36 (0.21-0.53) for benign IPNs with eight correctly downgraded intermediate-risk benign nodules and no malignant nodules misclassified into the low-risk category.
Conclusion: Incorporating LCP with select clinical variables results in an improvement in malignancy risk prediction and nodule classification and could reduce unnecessary invasive biopsies for IPNs.
期刊介绍:
BMJ Open Respiratory Research is a peer-reviewed, open access journal publishing respiratory and critical care medicine. It is the sister journal to Thorax and co-owned by the British Thoracic Society and BMJ. The journal focuses on robustness of methodology and scientific rigour with less emphasis on novelty or perceived impact. BMJ Open Respiratory Research operates a rapid review process, with continuous publication online, ensuring timely, up-to-date research is available worldwide. The journal publishes review articles and all research study types: Basic science including laboratory based experiments and animal models, Pilot studies or proof of concept, Observational studies, Study protocols, Registries, Clinical trials from phase I to multicentre randomised clinical trials, Systematic reviews and meta-analyses.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


