Nabih Berjaoui, Felix Santos, Fabiana Curti, Puiyee Sophia Chan, Savvas Lampridis, Akshay Patel, Andrea Bille
{"title":"Surgical management of complex mediastinitis: an 8-year single-centre experience reinforcing the role of open thoracotomy.","authors":"Nabih Berjaoui, Felix Santos, Fabiana Curti, Puiyee Sophia Chan, Savvas Lampridis, Akshay Patel, Andrea Bille","doi":"10.1093/icvts/ivaf154","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Mediastinitis is an infection affecting the mediastinum, often caused by cardiovascular or thoracic surgery procedures. Management entails antibiotic therapy, surgical debridement, drainage of infected sites and immediate or delayed closure. Negative pressure wound therapy is useful in cases of delayed sternal closure. Several approaches for mediastinal drainage have been proposed, but there is no consensus on the thoracic intervention approach.</p><p><strong>Methods: </strong>A single-centre, retrospective analysis from the UK analysed data from 19 patients who underwent surgical management for mediastinitis between September 2015 and April 2023. Our primary aim was to describe the outcomes from our series where we predominantly employed an open surgical approach.</p><p><strong>Results: </strong>The mean age of our cohort was 49 ± 17.12 years old; the mean performance status (PS ECOG) was 2 ± 0.77. Two people were known smokers (10.53%), while five were non-smokers (26.31%). Fifteen patients underwent an open operation (78.85%), with rest undergoing a minimally invasive approach. The majority of procedures were undertaken from the right-hand side. The overall intensive care unit admission rate was 68.42% (n = 13) with an in-hospital complication rate of 5.26% (n = 1). This was a respiratory arrest secondary to mucous plugging. There were no in-hospital deaths, and median follow-up was 41 months (22-50). Overall survival at 3 years was 85%.</p><p><strong>Conclusions: </strong>Open thoracotomy remains an important surgical strategy in the management of complex mediastinitis, but further validation is required through larger, prospective studies.</p>","PeriodicalId":73406,"journal":{"name":"Interdisciplinary cardiovascular and thoracic surgery","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-07-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12255885/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interdisciplinary cardiovascular and thoracic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/icvts/ivaf154","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"0","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Mediastinitis is an infection affecting the mediastinum, often caused by cardiovascular or thoracic surgery procedures. Management entails antibiotic therapy, surgical debridement, drainage of infected sites and immediate or delayed closure. Negative pressure wound therapy is useful in cases of delayed sternal closure. Several approaches for mediastinal drainage have been proposed, but there is no consensus on the thoracic intervention approach.
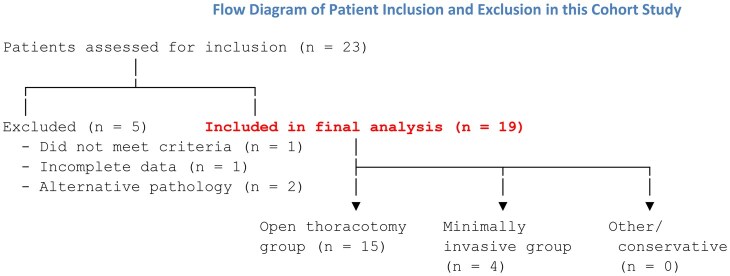
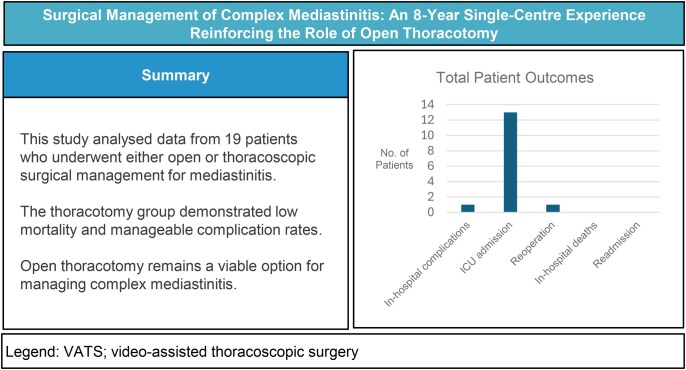
Methods: A single-centre, retrospective analysis from the UK analysed data from 19 patients who underwent surgical management for mediastinitis between September 2015 and April 2023. Our primary aim was to describe the outcomes from our series where we predominantly employed an open surgical approach.
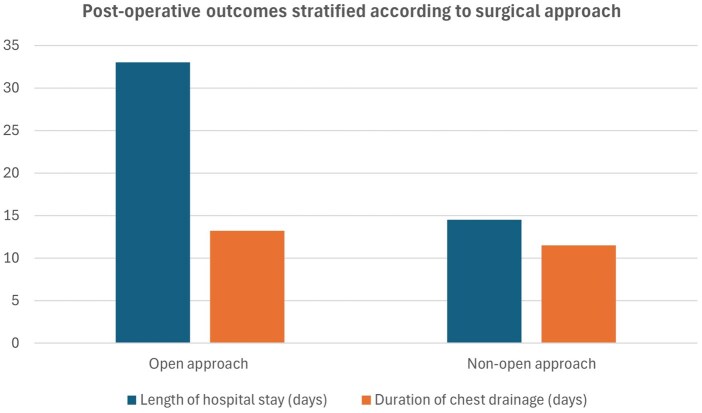
Results: The mean age of our cohort was 49 ± 17.12 years old; the mean performance status (PS ECOG) was 2 ± 0.77. Two people were known smokers (10.53%), while five were non-smokers (26.31%). Fifteen patients underwent an open operation (78.85%), with rest undergoing a minimally invasive approach. The majority of procedures were undertaken from the right-hand side. The overall intensive care unit admission rate was 68.42% (n = 13) with an in-hospital complication rate of 5.26% (n = 1). This was a respiratory arrest secondary to mucous plugging. There were no in-hospital deaths, and median follow-up was 41 months (22-50). Overall survival at 3 years was 85%.
Conclusions: Open thoracotomy remains an important surgical strategy in the management of complex mediastinitis, but further validation is required through larger, prospective studies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


