Ceilidh Welsh, Karl Harrison, Sara Lightowlers, Ian Gleeson, Alfred J W Beard, Emma Harris, Gillian C Barnett, Rajesh Jena
{"title":"A unified workflow for classifying patterns of locoregional failure using radiotherapy treatment planning dose distributions.","authors":"Ceilidh Welsh, Karl Harrison, Sara Lightowlers, Ian Gleeson, Alfred J W Beard, Emma Harris, Gillian C Barnett, Rajesh Jena","doi":"10.1093/bjro/tzaf007","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>This work describes a unified workflow for classifying patterns of locoregional recurrence (LRR) using radiotherapy planning dose distributions. This approach aims to incorporate dose parameters into LRR classifications and facilitate application across different treatment sites and dose prescriptions to standardise classification terminology.</p><p><strong>Methods: </strong>The relapse diagnostic CT (rCT) and manually delineated relapse gross tumour volume (rGTV) were co-registered with the radiotherapy planning CT (pCT) using deformable image registration (DIR). The DIR accuracy was quantified using the target registration error (TRE) using the absolute centroid distance between cancer site-specific regions of interest (ROIs). Dosimetric structures were delineated for planning regions receiving 95% of the dose prescribed to high-risk, intermediate-risk, and low-risk CTVs, relative to the cancer site or trial. The mapped rGTV was compared relative to each dose structure and classified into one of five categories: central and peripheral high-dose (Type A, Type B), central and peripheral elective-dose (Type C, Type D), and extraneous dose (Type E) failures.</p><p><strong>Results: </strong>The unified workflow was successfully implemented on two different patient use cases, one from the IMPORT HIGH breast cancer trial, one from the VoxTox head-and-neck study, classifying LRR as Type A and Type E failures, respectively.</p><p><strong>Conclusion: </strong>This workflow for classifying LRR is applicable across different cancer sites, despite differences in treatment protocol, target dose, and dose delivery. This provides a basis for utilising radiotherapy dose distributions to analyse patterns of failure irrespective of trial design or cancer-site.</p><p><strong>Advances in knowledge: </strong>Standardised classifications of LRR that are correlated with the planning dose distribution could provide insight into the underlying causes of LRR burden post-radiotherapy and allow for critical evaluation of the current concepts of defined clinical tumour volumes and optimal PTV dose regions.</p>","PeriodicalId":72419,"journal":{"name":"BJR open","volume":"7 1","pages":"tzaf007"},"PeriodicalIF":2.1000,"publicationDate":"2025-05-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12201982/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJR open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/bjro/tzaf007","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: This work describes a unified workflow for classifying patterns of locoregional recurrence (LRR) using radiotherapy planning dose distributions. This approach aims to incorporate dose parameters into LRR classifications and facilitate application across different treatment sites and dose prescriptions to standardise classification terminology.
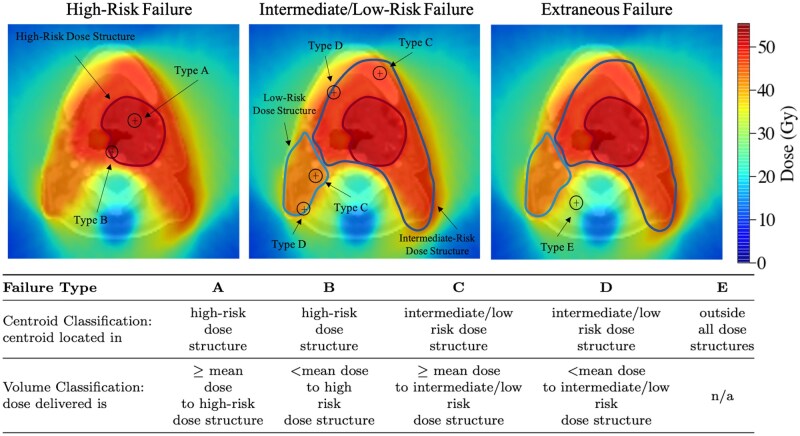
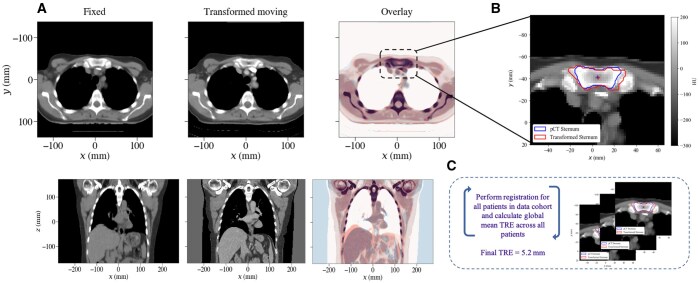
Methods: The relapse diagnostic CT (rCT) and manually delineated relapse gross tumour volume (rGTV) were co-registered with the radiotherapy planning CT (pCT) using deformable image registration (DIR). The DIR accuracy was quantified using the target registration error (TRE) using the absolute centroid distance between cancer site-specific regions of interest (ROIs). Dosimetric structures were delineated for planning regions receiving 95% of the dose prescribed to high-risk, intermediate-risk, and low-risk CTVs, relative to the cancer site or trial. The mapped rGTV was compared relative to each dose structure and classified into one of five categories: central and peripheral high-dose (Type A, Type B), central and peripheral elective-dose (Type C, Type D), and extraneous dose (Type E) failures.
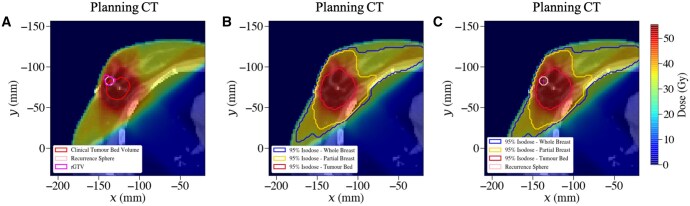
Results: The unified workflow was successfully implemented on two different patient use cases, one from the IMPORT HIGH breast cancer trial, one from the VoxTox head-and-neck study, classifying LRR as Type A and Type E failures, respectively.
Conclusion: This workflow for classifying LRR is applicable across different cancer sites, despite differences in treatment protocol, target dose, and dose delivery. This provides a basis for utilising radiotherapy dose distributions to analyse patterns of failure irrespective of trial design or cancer-site.
Advances in knowledge: Standardised classifications of LRR that are correlated with the planning dose distribution could provide insight into the underlying causes of LRR burden post-radiotherapy and allow for critical evaluation of the current concepts of defined clinical tumour volumes and optimal PTV dose regions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


