{"title":"Descending Necrotizing Mediastinitis as a Deadly Complication Following Laparoscopic Sleeve Gastrectomy: A Case Report.","authors":"Kengo Kadoya, Kotaro Wakamatsu","doi":"10.70352/scrj.cr.25-0213","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Laparoscopic sleeve gastrectomy is a standard and safe surgical procedure for patients with morbid obesity. A potential complication is piriform fossa injury, which can occur during calibration tube insertion. We encountered a case of descending necrotizing mediastinitis, a serious and progressive infection originating from a piriform fossa injury that was potentially exacerbated by diabetes.</p><p><strong>Case presentation: </strong>A female patient with morbid obesity (body mass index, 41 kg/m<sup>2</sup>) and a heavy smoking habit underwent laparoscopic sleeve gastrectomy and was discharged without any immediate postoperative complications. Six weeks later, the patient presented with severe chest and back pain that required continuous fentanyl injection for pain management. Initially, staple line leakage, commonly observed after sleeve gastrectomy, was suspected. However, her condition progressively worsened, and she was admitted to the ICU. An enhanced abdominal CT scan extending to the cervical region revealed a cervical abscess extending to the lower mediastinal region. The patient was diagnosed with descending necrotizing mediastinitis. Given the rarity of this disease, we hypothesized that her smoking habits exacerbated the piriform fossa injury caused by the calibration tube used during gastrectomy. Following the diagnosis, emergency abscess drainage surgery was performed, and the patient was successfully treated.</p><p><strong>Conclusions: </strong>This is the 1st reported case of descending necrotizing mediastinitis as a fatal complication of laparoscopic sleeve gastrectomy, which was identified and treated successfully owing to the timely and expanded use of an enhanced CT scan that included the cervical region. Traditionally, the cervical area has not been routinely examined when diagnosing complications following abdominal surgery, underscoring the importance of a comprehensive imaging approach from the neck to the abdomen to detect complications after sleeve gastrectomy.</p>","PeriodicalId":22096,"journal":{"name":"Surgical Case Reports","volume":"11 1","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12197851/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.70352/scrj.cr.25-0213","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/21 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Laparoscopic sleeve gastrectomy is a standard and safe surgical procedure for patients with morbid obesity. A potential complication is piriform fossa injury, which can occur during calibration tube insertion. We encountered a case of descending necrotizing mediastinitis, a serious and progressive infection originating from a piriform fossa injury that was potentially exacerbated by diabetes.
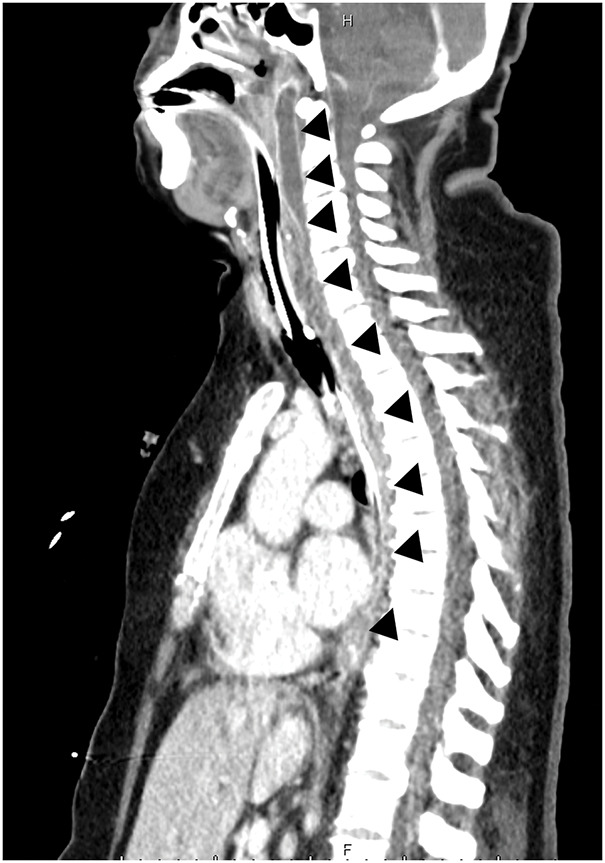
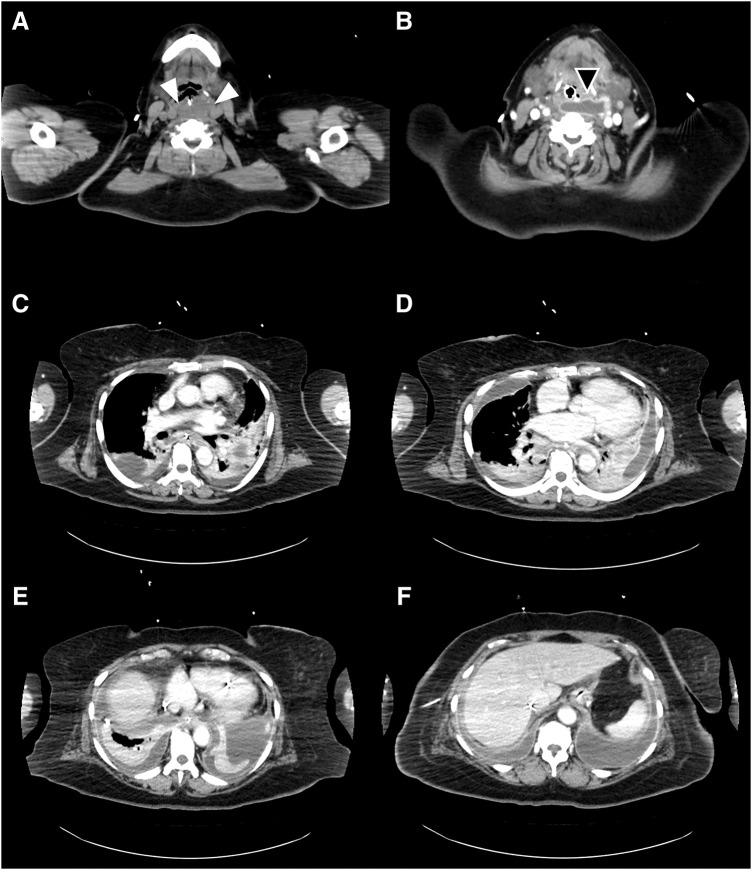
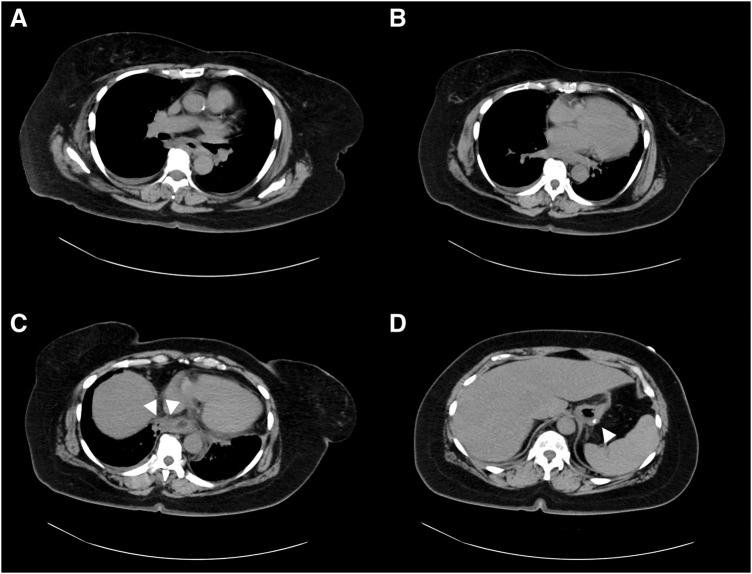
Case presentation: A female patient with morbid obesity (body mass index, 41 kg/m2) and a heavy smoking habit underwent laparoscopic sleeve gastrectomy and was discharged without any immediate postoperative complications. Six weeks later, the patient presented with severe chest and back pain that required continuous fentanyl injection for pain management. Initially, staple line leakage, commonly observed after sleeve gastrectomy, was suspected. However, her condition progressively worsened, and she was admitted to the ICU. An enhanced abdominal CT scan extending to the cervical region revealed a cervical abscess extending to the lower mediastinal region. The patient was diagnosed with descending necrotizing mediastinitis. Given the rarity of this disease, we hypothesized that her smoking habits exacerbated the piriform fossa injury caused by the calibration tube used during gastrectomy. Following the diagnosis, emergency abscess drainage surgery was performed, and the patient was successfully treated.
Conclusions: This is the 1st reported case of descending necrotizing mediastinitis as a fatal complication of laparoscopic sleeve gastrectomy, which was identified and treated successfully owing to the timely and expanded use of an enhanced CT scan that included the cervical region. Traditionally, the cervical area has not been routinely examined when diagnosing complications following abdominal surgery, underscoring the importance of a comprehensive imaging approach from the neck to the abdomen to detect complications after sleeve gastrectomy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


