Saima Ahmed, Tabassum Elahi, Muhammed Mubarak, Ejaz Ahmed
{"title":"Clinicopathological characteristics and long-term outcomes of adult patients with proliferative lupus nephritis.","authors":"Saima Ahmed, Tabassum Elahi, Muhammed Mubarak, Ejaz Ahmed","doi":"10.5527/wjn.v14.i2.102713","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Proliferative lupus nephritis (PLN) is the most severe form of lupus nephritis (LN). There are limited data available on renal outcomes of PLN from developing countries.</p><p><strong>Aim: </strong>To determine the clinicopathological characteristics and long-term outcomes in terms of remission, requirement of kidney replacement therapy (KRT), and patient survival.</p><p><strong>Methods: </strong>A retrospective analysis was conducted on biopsy-proven focal or diffuse PLN cases diagnosed between 1998 and 2019 at the Sindh Institute of Urology and Transplantation and followed up at the renal clinic for a minimum of 5 years. All patients were induced with a combination of intravenous cyclophosphamide and corticosteroids for 6 months, followed by maintenance treatment with azathioprine (AZA) or mycophenolate mofetil (MMF). Data were analyzed using Statistical Package for the Social Sciences, version 22.0. <i>P</i> ≤ 0.05 was considered statistically significant.</p><p><strong>Results: </strong>The mean age at the onset of systemic lupus erythematosus was 24.12 years ± 8.89 years, and at LN onset, 26.63 years ± 8.61 years. There was a female predominance of 184 (88.9%) cases. Among baseline characteristics, reduced estimated glomerular filtration rate, presence of hypertension, requirement of KRT, and underlying renal histology (International Society of Nephrology/Renal Pathology Society class IV than class III) were significantly associated with end-stage kidney disease (ESKD) and mortality. The renal outcomes were negatively correlated with age, duration of symptoms, and 24-hour urinary protein excretion. The overall remission rate was 89.8% at the end of induction therapy. At 5 years, 141 (68.11%) patients were in complete and partial remission (94 [45.4%] and 47 [22.7%], respectively). In total, 19 (9.2%) patients required KRT on presentation, and at 5 years, 38 (18.4%) patients developed ESKD, and 28 (13.5%) patients died. Thirty-four (16.4%) patients had a renal relapse, more with AZA than MMF (30 [88.2%] <i>vs</i> 4 [11.76%], respectively; <i>P</i> = 0.04). Renal survival at 6 months was 89.8%, while at 5 years, it was 68.11%, showing a significant improvement in patients who did not need KRT at the time of presentation (<i>P</i> < 0.0001).</p><p><strong>Conclusion: </strong>Baseline renal functions, requirement of KRT, and diffuse proliferative disease were the most relevant prognostic factors for kidney survival among this cohort. Short-term renal outcomes were good. Long-term outcomes were poorer with AZA-based maintenance therapy than with MMF, with more ESKD and mortality.</p>","PeriodicalId":94272,"journal":{"name":"World journal of nephrology","volume":"14 2","pages":"102713"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12001224/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World journal of nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5527/wjn.v14.i2.102713","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Proliferative lupus nephritis (PLN) is the most severe form of lupus nephritis (LN). There are limited data available on renal outcomes of PLN from developing countries.
Aim: To determine the clinicopathological characteristics and long-term outcomes in terms of remission, requirement of kidney replacement therapy (KRT), and patient survival.
Methods: A retrospective analysis was conducted on biopsy-proven focal or diffuse PLN cases diagnosed between 1998 and 2019 at the Sindh Institute of Urology and Transplantation and followed up at the renal clinic for a minimum of 5 years. All patients were induced with a combination of intravenous cyclophosphamide and corticosteroids for 6 months, followed by maintenance treatment with azathioprine (AZA) or mycophenolate mofetil (MMF). Data were analyzed using Statistical Package for the Social Sciences, version 22.0. P ≤ 0.05 was considered statistically significant.
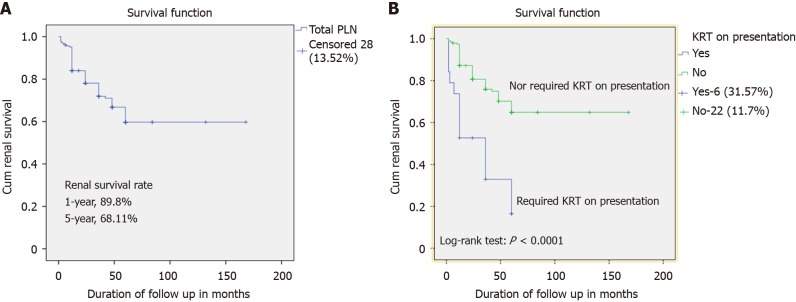
Results: The mean age at the onset of systemic lupus erythematosus was 24.12 years ± 8.89 years, and at LN onset, 26.63 years ± 8.61 years. There was a female predominance of 184 (88.9%) cases. Among baseline characteristics, reduced estimated glomerular filtration rate, presence of hypertension, requirement of KRT, and underlying renal histology (International Society of Nephrology/Renal Pathology Society class IV than class III) were significantly associated with end-stage kidney disease (ESKD) and mortality. The renal outcomes were negatively correlated with age, duration of symptoms, and 24-hour urinary protein excretion. The overall remission rate was 89.8% at the end of induction therapy. At 5 years, 141 (68.11%) patients were in complete and partial remission (94 [45.4%] and 47 [22.7%], respectively). In total, 19 (9.2%) patients required KRT on presentation, and at 5 years, 38 (18.4%) patients developed ESKD, and 28 (13.5%) patients died. Thirty-four (16.4%) patients had a renal relapse, more with AZA than MMF (30 [88.2%] vs 4 [11.76%], respectively; P = 0.04). Renal survival at 6 months was 89.8%, while at 5 years, it was 68.11%, showing a significant improvement in patients who did not need KRT at the time of presentation (P < 0.0001).
Conclusion: Baseline renal functions, requirement of KRT, and diffuse proliferative disease were the most relevant prognostic factors for kidney survival among this cohort. Short-term renal outcomes were good. Long-term outcomes were poorer with AZA-based maintenance therapy than with MMF, with more ESKD and mortality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


