Ritwik Dey, Lakshmi Kattamuri, Yagnapriya Chirrareddy, Eder Luna Ceron, Kunal Sharma, Osvaldo Padilla, Abhizith Deoker
{"title":"Lofgren's Syndrome: A Unique Presentation of Sarcoidosis Masquerading as Lower Extremity Cellulitis.","authors":"Ritwik Dey, Lakshmi Kattamuri, Yagnapriya Chirrareddy, Eder Luna Ceron, Kunal Sharma, Osvaldo Padilla, Abhizith Deoker","doi":"10.1177/23247096251352366","DOIUrl":null,"url":null,"abstract":"<p><p>Löfgren's syndrome is an acute, self-limiting variant of sarcoidosis, typically presenting with erythema nodosum, bilateral hilar lymphadenopathy, and acute arthritis or periarthritis-most commonly involving the ankles. Its clinical overlap with other inflammatory conditions can pose a diagnostic challenge. We describe a 34-year-old male with no prior medical history who presented with bilateral ankle and foot pain, erythema, and swelling, initially diagnosed as cellulitis based on imaging findings. He has no response to broad-spectrum antibiotics. During his further hospital stay, he developed polyarthritis. Laboratory evaluation revealed neutrophilic leukocytosis, elevated inflammatory markers, and a normal serum angiotensin-converting enzyme level. Imaging showed bilateral hilar lymphadenopathy and intra-abdominal adenopathy. Bronchoscopy with bronchoalveolar lavage revealed an elevated CD4:CD8 ratio (5.0), and endobronchial ultrasound-guided transbronchial needle aspiration confirmed noncaseating granulomas. Infectious, autoimmune, and malignant causes were excluded. Based on clinical features and histology, a diagnosis of Löfgren's syndrome was established. Nonsteroidal anti-inflammatory drug therapy led to rapid clinical improvement, and antibiotics were discontinued. Löfgren's syndrome should be considered in patients presenting with bilateral lower extremity erythema and swelling unresponsive to antibiotics, especially when accompanied by systemic symptoms. Early thoracic imaging and consideration of sarcoidosis in the differential diagnosis can prevent misdiagnosis and unnecessary treatment.</p>","PeriodicalId":16198,"journal":{"name":"Journal of investigative medicine high impact case reports","volume":"13 ","pages":"23247096251352366"},"PeriodicalIF":0.8000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12202904/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of investigative medicine high impact case reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23247096251352366","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/26 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
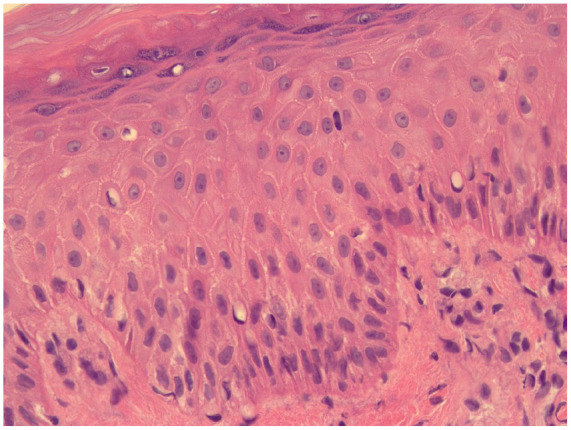
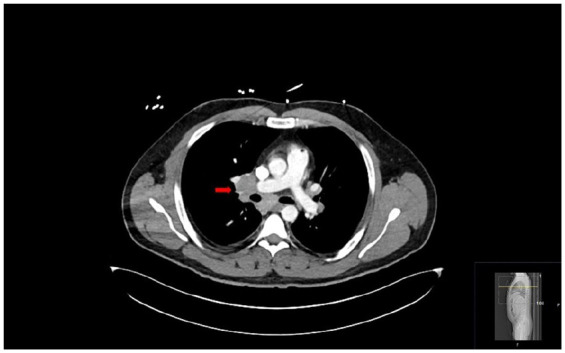
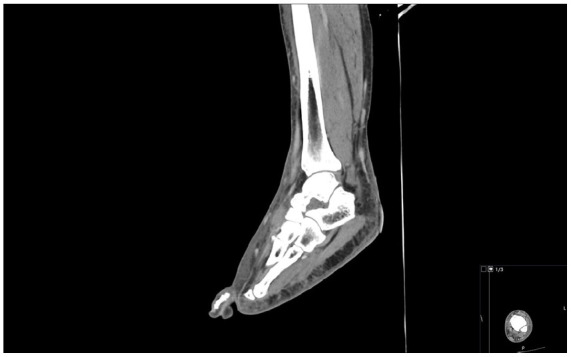
Löfgren's syndrome is an acute, self-limiting variant of sarcoidosis, typically presenting with erythema nodosum, bilateral hilar lymphadenopathy, and acute arthritis or periarthritis-most commonly involving the ankles. Its clinical overlap with other inflammatory conditions can pose a diagnostic challenge. We describe a 34-year-old male with no prior medical history who presented with bilateral ankle and foot pain, erythema, and swelling, initially diagnosed as cellulitis based on imaging findings. He has no response to broad-spectrum antibiotics. During his further hospital stay, he developed polyarthritis. Laboratory evaluation revealed neutrophilic leukocytosis, elevated inflammatory markers, and a normal serum angiotensin-converting enzyme level. Imaging showed bilateral hilar lymphadenopathy and intra-abdominal adenopathy. Bronchoscopy with bronchoalveolar lavage revealed an elevated CD4:CD8 ratio (5.0), and endobronchial ultrasound-guided transbronchial needle aspiration confirmed noncaseating granulomas. Infectious, autoimmune, and malignant causes were excluded. Based on clinical features and histology, a diagnosis of Löfgren's syndrome was established. Nonsteroidal anti-inflammatory drug therapy led to rapid clinical improvement, and antibiotics were discontinued. Löfgren's syndrome should be considered in patients presenting with bilateral lower extremity erythema and swelling unresponsive to antibiotics, especially when accompanied by systemic symptoms. Early thoracic imaging and consideration of sarcoidosis in the differential diagnosis can prevent misdiagnosis and unnecessary treatment.
期刊介绍:
The AFMR is committed to enhancing the training and career development of our members and to furthering its mission to facilitate the conduct of research to improve medical care. Case reports represent an important avenue for trainees (interns, residents, and fellows) and early-stage faculty to demonstrate productive, scholarly activity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


