Marianne Kruse, Ida Katinka Lenz, David Josuttis, Philip Plettig, Klaus Hahnenkamp, Denis Gümbel, Claas Güthoff, Bernd Hartmann, Martin Aman, Marc Dominik Schmittner, Volker Gebhardt
{"title":"Characterisation of Fluid Administration in Burn Shock-A Retrospective Cohort Analysis.","authors":"Marianne Kruse, Ida Katinka Lenz, David Josuttis, Philip Plettig, Klaus Hahnenkamp, Denis Gümbel, Claas Güthoff, Bernd Hartmann, Martin Aman, Marc Dominik Schmittner, Volker Gebhardt","doi":"10.3390/ebj6020035","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Finding the optimal amount of fluid is a major challenge in burn shock. Although there is evidence that a restrictive fluid regime is beneficial, current practice shows fluid resuscitation still well above recommendations. The extent of trauma, pre-hospital care and the patient's pre-existing conditions influence requirements.</p><p><strong>Methods: </strong>We analysed outcomes and influencing factors of fluid regimes in a retrospective cohort study including 90 severely burnt patients resuscitated with the same protocol.</p><p><strong>Results: </strong>The mean amount of fluids in the first 24 h was 6.5 mL/kg bodyweight (BW)/% total burn surface area (TBSA). A total of 14% received restrictive (<4), 34% received liberal (4-6) and 51% received excessive (>6) mL/kgBW/%TBSA fluids. There was no difference regarding mortality, age, complications, organ failure, inhalation injury or full-thickness burns in the groups. Patients with excessive fluid therapy had a significantly lower ABSI score (9 vs. 11, <i>p</i> = 0.05) and TBSA (35 vs. 51%, <i>p</i> < 0.001), while patients with a restrictive fluid therapy needed fewer incidences of surgery to cover burn wounds (3.5 vs. 9.0 vs. 7.0, <i>p</i> = 0.008). History of liver disease or alcohol abuse tended to indicate excessive fluid administration. Patients with pre-existing heart failure received restrictive fluid therapy (23 vs. 3 vs. 4%, <i>p</i> = 0.03).</p><p><strong>Conclusions: </strong>Individualised, timely therapy monitoring is as essential as identifying patients with a higher or lower fluid requirement. Excessive fluid resuscitation had fewer deleterious consequences in complications than expected but seems to influence wound healing. Awareness of circumstances that prompt deviations from recommended fluid rates remains elementary.</p>","PeriodicalId":72961,"journal":{"name":"European burn journal","volume":"6 2","pages":""},"PeriodicalIF":1.2000,"publicationDate":"2025-06-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12191774/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European burn journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/ebj6020035","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Finding the optimal amount of fluid is a major challenge in burn shock. Although there is evidence that a restrictive fluid regime is beneficial, current practice shows fluid resuscitation still well above recommendations. The extent of trauma, pre-hospital care and the patient's pre-existing conditions influence requirements.
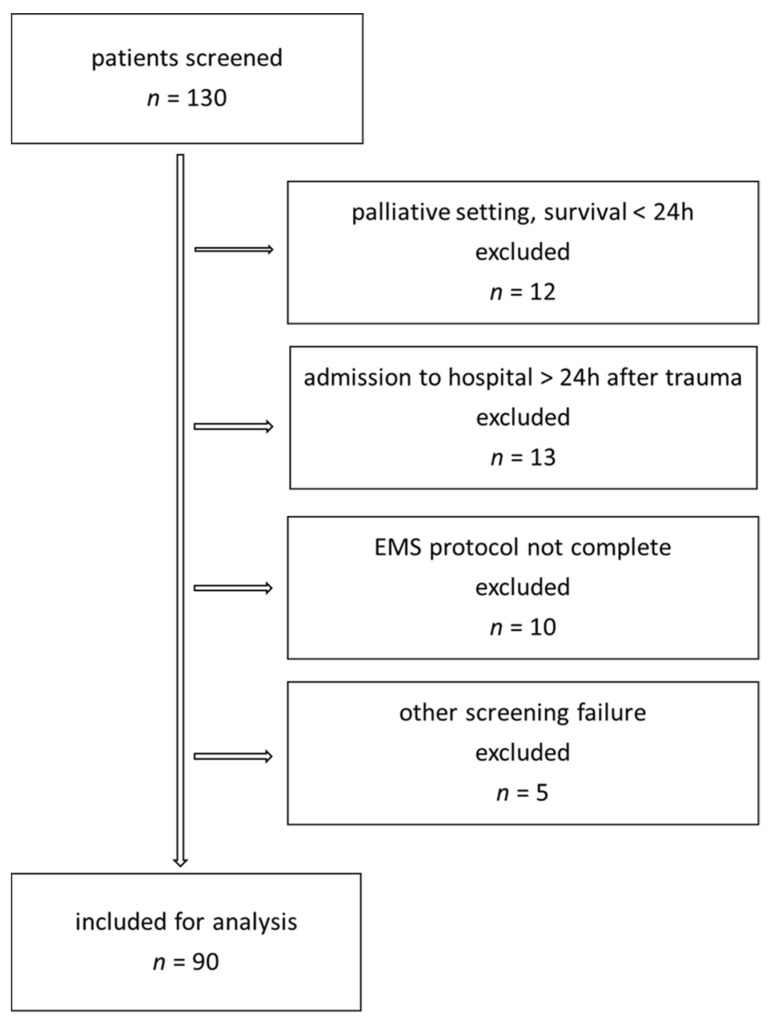
Methods: We analysed outcomes and influencing factors of fluid regimes in a retrospective cohort study including 90 severely burnt patients resuscitated with the same protocol.
Results: The mean amount of fluids in the first 24 h was 6.5 mL/kg bodyweight (BW)/% total burn surface area (TBSA). A total of 14% received restrictive (<4), 34% received liberal (4-6) and 51% received excessive (>6) mL/kgBW/%TBSA fluids. There was no difference regarding mortality, age, complications, organ failure, inhalation injury or full-thickness burns in the groups. Patients with excessive fluid therapy had a significantly lower ABSI score (9 vs. 11, p = 0.05) and TBSA (35 vs. 51%, p < 0.001), while patients with a restrictive fluid therapy needed fewer incidences of surgery to cover burn wounds (3.5 vs. 9.0 vs. 7.0, p = 0.008). History of liver disease or alcohol abuse tended to indicate excessive fluid administration. Patients with pre-existing heart failure received restrictive fluid therapy (23 vs. 3 vs. 4%, p = 0.03).
Conclusions: Individualised, timely therapy monitoring is as essential as identifying patients with a higher or lower fluid requirement. Excessive fluid resuscitation had fewer deleterious consequences in complications than expected but seems to influence wound healing. Awareness of circumstances that prompt deviations from recommended fluid rates remains elementary.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


