A Comparison of All-Cause Mortality in Patients Who Required Glaucoma Surgery for Neovascular Glaucoma or Primary Open-Angle Glaucoma: A Retrospective Cohort Study.
Laura D Palmer, Levi D Kauffman, Gregory B Russell, Atalie C Thompson, Gillian G Treadwell
{"title":"A Comparison of All-Cause Mortality in Patients Who Required Glaucoma Surgery for Neovascular Glaucoma or Primary Open-Angle Glaucoma: A Retrospective Cohort Study.","authors":"Laura D Palmer, Levi D Kauffman, Gregory B Russell, Atalie C Thompson, Gillian G Treadwell","doi":"10.3390/vision9020049","DOIUrl":null,"url":null,"abstract":"<p><p>This retrospective review examines whether there is a difference in all-cause mortality in patients who required surgical intervention for neovascular glaucoma (NVG, N = 186) versus primary open-angle glaucoma (POAG, N = 190). Cox proportional hazard models compared mortality across three models: unadjusted, age-adjusted (Model 1), and age-, hypertension-, and diabetes-adjusted (Model 2). In all models, NVG patients who required glaucoma surgery had a higher all-cause mortality rate compared to those with POAG who underwent similar procedures: unadjusted (HR 2.22, (1.59, 3.10), <i>p</i> < 0.0001), Model 1 (HR 2.99, 95% CI (2.12, 4.22), <i>p</i> < 0.0001), and Model 2 (HR 1.88, 95% CI (1.27, 2.80), <i>p</i> < 0.0018). In Model 1, those with NVG due to PDR had a higher all-cause mortality rate after glaucoma surgery than those with NVG secondary to CRVO (HR 2.00, 95% CI (1.19, 3.45), <i>p</i> < 0.0095). Patients treated with CPC had higher all-cause mortality rates than those treated with tube shunt in all models: unadjusted (HR 1.82, 95% CI (1.33, 2.47), <i>p</i> < 0.0001), Model 1 (HR 1.91, 95% CI (1.40, 2.61), <i>p</i> < 0.0001), and Model 2 (HR 1.50, 95% CI (1.04, 2.16), <i>p</i> < 0.03). We observed a higher all-cause mortality rate among patients with NVG requiring glaucoma surgery compared to those with POAG requiring similar surgeries, which could suggest that NVG patients requiring glaucoma surgery had more compromised systemic health.</p>","PeriodicalId":36586,"journal":{"name":"Vision (Switzerland)","volume":"9 2","pages":""},"PeriodicalIF":1.8000,"publicationDate":"2025-06-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12197471/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Vision (Switzerland)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/vision9020049","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
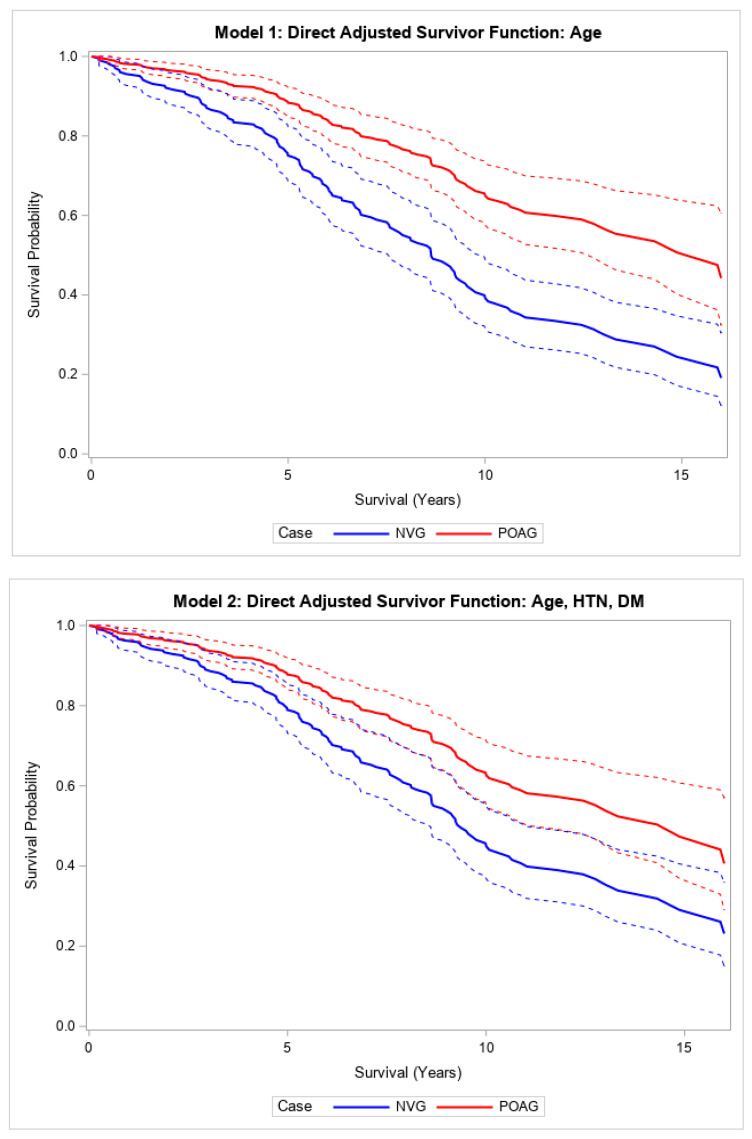
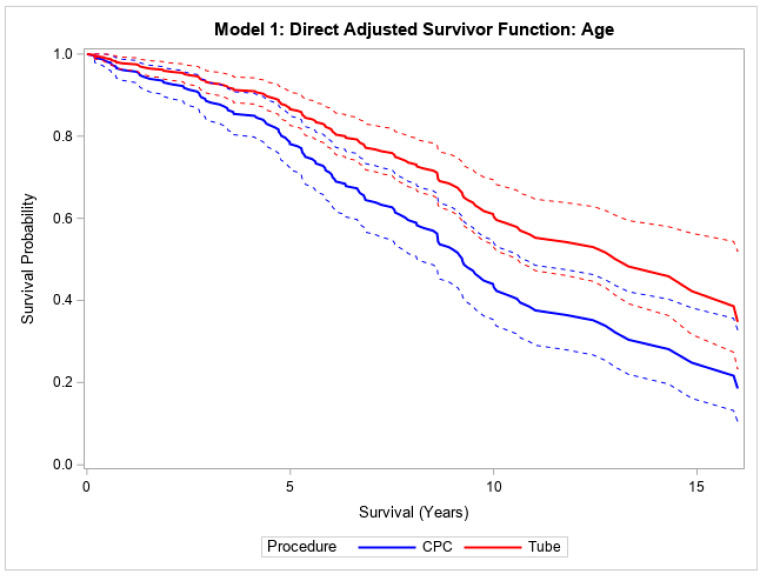
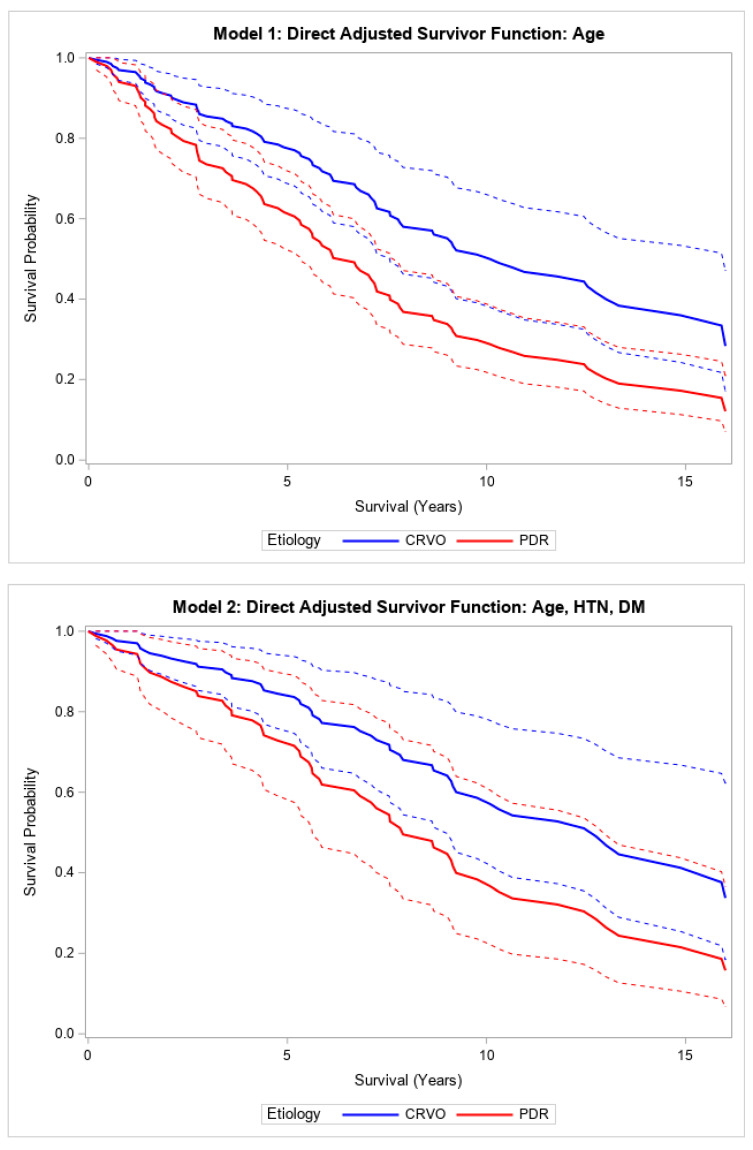
This retrospective review examines whether there is a difference in all-cause mortality in patients who required surgical intervention for neovascular glaucoma (NVG, N = 186) versus primary open-angle glaucoma (POAG, N = 190). Cox proportional hazard models compared mortality across three models: unadjusted, age-adjusted (Model 1), and age-, hypertension-, and diabetes-adjusted (Model 2). In all models, NVG patients who required glaucoma surgery had a higher all-cause mortality rate compared to those with POAG who underwent similar procedures: unadjusted (HR 2.22, (1.59, 3.10), p < 0.0001), Model 1 (HR 2.99, 95% CI (2.12, 4.22), p < 0.0001), and Model 2 (HR 1.88, 95% CI (1.27, 2.80), p < 0.0018). In Model 1, those with NVG due to PDR had a higher all-cause mortality rate after glaucoma surgery than those with NVG secondary to CRVO (HR 2.00, 95% CI (1.19, 3.45), p < 0.0095). Patients treated with CPC had higher all-cause mortality rates than those treated with tube shunt in all models: unadjusted (HR 1.82, 95% CI (1.33, 2.47), p < 0.0001), Model 1 (HR 1.91, 95% CI (1.40, 2.61), p < 0.0001), and Model 2 (HR 1.50, 95% CI (1.04, 2.16), p < 0.03). We observed a higher all-cause mortality rate among patients with NVG requiring glaucoma surgery compared to those with POAG requiring similar surgeries, which could suggest that NVG patients requiring glaucoma surgery had more compromised systemic health.
本回顾性研究探讨了新生血管性青光眼(NVG, N = 186)与原发性开角型青光眼(POAG, N = 190)患者的全因死亡率是否存在差异。Cox比例风险模型比较了三种模型的死亡率:未调整、年龄调整(模型1)和年龄、高血压和糖尿病调整(模型2)。在所有模型中,与接受类似手术的POAG患者相比,需要青光眼手术的NVG患者的全因死亡率更高:未调整(HR 2.22, (1.59, 3.10), p < 0.0001),模型1 (HR 2.99, 95% CI (2.12, 4.22), p < 0.0001),模型2 (HR 1.88, 95% CI (1.27, 2.80), p < 0.0018)。模型1中,PDR致NVG患者术后全因死亡率高于CRVO继发NVG患者(HR 2.00, 95% CI (1.19, 3.45), p < 0.0095)。在所有模型中,CPC治疗的患者的全因死亡率高于分流治疗的患者:未调整(HR 1.82, 95% CI (1.33, 2.47), p < 0.0001),模型1 (HR 1.91, 95% CI (1.40, 2.61), p < 0.0001),模型2 (HR 1.50, 95% CI (1.04, 2.16), p < 0.03)。我们观察到,与需要类似手术的POAG患者相比,需要青光眼手术的NVG患者的全因死亡率更高,这可能表明需要青光眼手术的NVG患者有更多的全身健康受损。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


