{"title":"Beyond Inflammatory Bowel Disease: Calprotectin as a Marker for Trichobezoar? A Case Report.","authors":"Ammar Khayat","doi":"10.1159/000546623","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Trichobezoar is an aggregation of swallowed hair strands that entangle in the stomach. It presents with abdominal pain, vomiting, and diarrhea. Diagnosis is usually made by imaging and endoscopy. Surgical removal is typically required, but endoscopic retrieval has been successful. Fecal calprotectin is a biomarker of inflammation that is typically elevated in inflammatory bowel disease (IBD) but is also elevated in other gastrointestinal (GI) disorders such as infections. Trichobezoar is not known to precipitate GI inflammation and has never been reported among the etiologies of elevated fecal calprotectin. Herein is a case presenting with vague abdominal pain and elevated fecal calprotectin that was attributed solely to a trichobezoar.</p><p><strong>Case presentation: </strong>A 7-year-old girl presented with abdominal pain for 6 months associated with occasional vomiting and diarrhea. Family history was positive for ulcerative colitis. Physical examination was unremarkable including normal growth. Diagnostic workup revealed elevated fecal calprotectin at 433.9 mg/kg. Upper and lower endoscopies were performed. A trichobezoar with Rapunzel syndrome was incidentally found in the stomach extending into the duodenum without frank obstruction. Histology showed reactive gastropathy in a few areas of mechanical rubbing by hair strands; otherwise, it was completely unremarkable in both upper and lower GI biopsies. Endoscopic retrieval of piecemeal hair locks was done. Surgical removal was subsequently done due to the generous size of the mass.</p><p><strong>Conclusion: </strong>Fecal calprotectin is an important biomarker for IBD, as well as other unusual GI pathologies, and clinical context is crucial when interpreting its value.</p>","PeriodicalId":9614,"journal":{"name":"Case Reports in Gastroenterology","volume":"19 1","pages":"482-487"},"PeriodicalIF":0.6000,"publicationDate":"2025-06-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12187109/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000546623","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Trichobezoar is an aggregation of swallowed hair strands that entangle in the stomach. It presents with abdominal pain, vomiting, and diarrhea. Diagnosis is usually made by imaging and endoscopy. Surgical removal is typically required, but endoscopic retrieval has been successful. Fecal calprotectin is a biomarker of inflammation that is typically elevated in inflammatory bowel disease (IBD) but is also elevated in other gastrointestinal (GI) disorders such as infections. Trichobezoar is not known to precipitate GI inflammation and has never been reported among the etiologies of elevated fecal calprotectin. Herein is a case presenting with vague abdominal pain and elevated fecal calprotectin that was attributed solely to a trichobezoar.
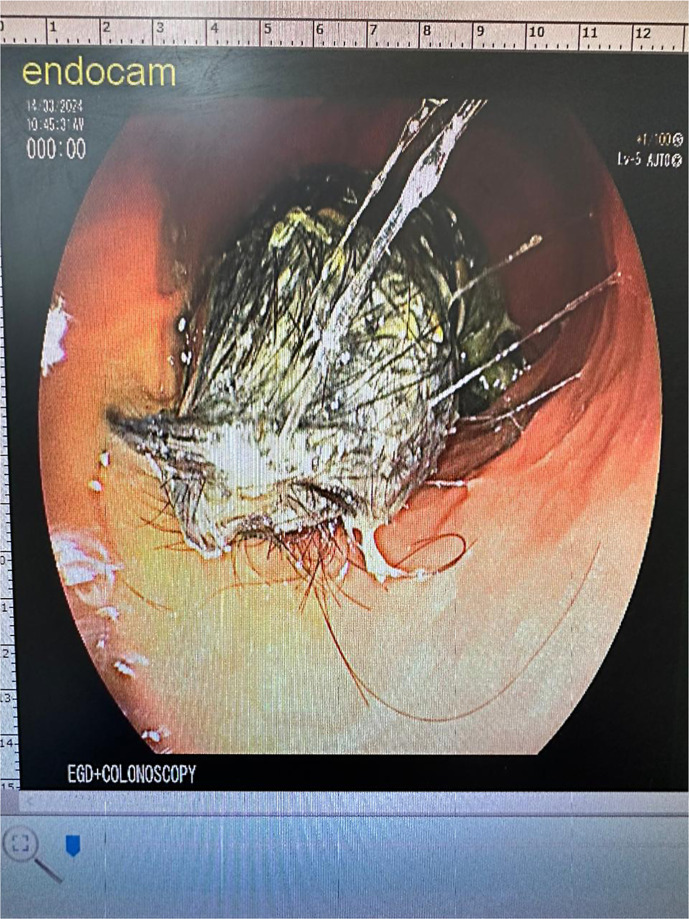
Case presentation: A 7-year-old girl presented with abdominal pain for 6 months associated with occasional vomiting and diarrhea. Family history was positive for ulcerative colitis. Physical examination was unremarkable including normal growth. Diagnostic workup revealed elevated fecal calprotectin at 433.9 mg/kg. Upper and lower endoscopies were performed. A trichobezoar with Rapunzel syndrome was incidentally found in the stomach extending into the duodenum without frank obstruction. Histology showed reactive gastropathy in a few areas of mechanical rubbing by hair strands; otherwise, it was completely unremarkable in both upper and lower GI biopsies. Endoscopic retrieval of piecemeal hair locks was done. Surgical removal was subsequently done due to the generous size of the mass.
Conclusion: Fecal calprotectin is an important biomarker for IBD, as well as other unusual GI pathologies, and clinical context is crucial when interpreting its value.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


