{"title":"Long-Term Outcomes in Patients With Non-Ampullary Duodenal Neuroendocrine Tumors.","authors":"Da-Bin Jeong, Sang-Gyun Kim, Soo-Jeong Cho","doi":"10.7704/kjhugr.2025.0008","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Although non-ampullary duodenal neuroendocrine tumors (NADNETs) are rare neoplasms, their incidence has been increasing. In this study, we aimed to analyze the long-term outcomes of patients with NADNETs who underwent endoscopic resection (ER) or surgery.</p><p><strong>Methods: </strong>This retrospective study included 55 adults (aged 26-78 years) diagnosed with NADNETs between 2009 and 2022 at Seoul National University Hospital. We categorized the patients into 3 groups: 21 underwent ER, 28 underwent surgical resection, and 6 had no detectable residual tumors after the initial biopsy during the follow-up period. Continuous data were examined using the Mann-Whitney U or Kruskal-Wallis tests, and categorical variables were analyzed using the χ2 or Fisher's exact tests.</p><p><strong>Results: </strong>A total of 21 patients, with a mean tumor size of 9.2±5.3 mm, underwent successful ER. After ER, three patients experienced perforation (14% [3/21]); two underwent primary repair surgery, and one recovered with conservative treatment. The mean tumor size of 28 patients who underwent surgical resection was 13.9±6.7 mm. There were no cases of postoperative bleeding or perforation; however, four patients experienced ileus and required prolonged hospital stays. The median follow-up periods for patients who underwent ER, surgical resection, and removal after the initial biopsy were 42, 48, and 42.5 months, respectively. During the follow-up period, no recurrence was observed in any group.</p><p><strong>Conclusions: </strong>Recurrence-free survival in patients undergoing ER for NADNETs, with an endoscopically measured size of approximately 10 mm, was comparable to that of patients undergoing surgical resection. However, ER carried a relatively high risk of perforation due to the challenging anatomical access and thin duodenal wall.</p>","PeriodicalId":520887,"journal":{"name":"The Korean journal of helicobacter and upper gastrointestinal research","volume":"25 1","pages":"54-63"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12173577/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Korean journal of helicobacter and upper gastrointestinal research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7704/kjhugr.2025.0008","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/7 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Although non-ampullary duodenal neuroendocrine tumors (NADNETs) are rare neoplasms, their incidence has been increasing. In this study, we aimed to analyze the long-term outcomes of patients with NADNETs who underwent endoscopic resection (ER) or surgery.
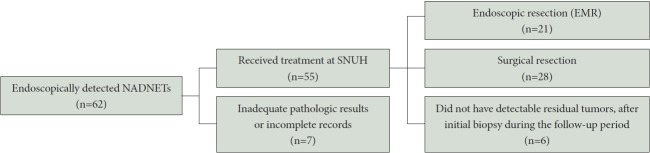
Methods: This retrospective study included 55 adults (aged 26-78 years) diagnosed with NADNETs between 2009 and 2022 at Seoul National University Hospital. We categorized the patients into 3 groups: 21 underwent ER, 28 underwent surgical resection, and 6 had no detectable residual tumors after the initial biopsy during the follow-up period. Continuous data were examined using the Mann-Whitney U or Kruskal-Wallis tests, and categorical variables were analyzed using the χ2 or Fisher's exact tests.
Results: A total of 21 patients, with a mean tumor size of 9.2±5.3 mm, underwent successful ER. After ER, three patients experienced perforation (14% [3/21]); two underwent primary repair surgery, and one recovered with conservative treatment. The mean tumor size of 28 patients who underwent surgical resection was 13.9±6.7 mm. There were no cases of postoperative bleeding or perforation; however, four patients experienced ileus and required prolonged hospital stays. The median follow-up periods for patients who underwent ER, surgical resection, and removal after the initial biopsy were 42, 48, and 42.5 months, respectively. During the follow-up period, no recurrence was observed in any group.
Conclusions: Recurrence-free survival in patients undergoing ER for NADNETs, with an endoscopically measured size of approximately 10 mm, was comparable to that of patients undergoing surgical resection. However, ER carried a relatively high risk of perforation due to the challenging anatomical access and thin duodenal wall.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


