Julia M Balboni, Karthik Madhira, Victor Martinez, Wei-Shao Tung, John G Kennedy, Arianna L Gianakos
{"title":"Effect of blood flow restriction on muscle strength and stability following foot and ankle injury: A systematic review.","authors":"Julia M Balboni, Karthik Madhira, Victor Martinez, Wei-Shao Tung, John G Kennedy, Arianna L Gianakos","doi":"10.5312/wjo.v16.i6.106804","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Poor musculoskeletal recovery following foot and ankle injury can result in chronic instability and persistent muscle weakness. Preliminary evidence has shown that blood flow restriction (BFR) rehabilitation can increase muscle strength and stability, helping to restore physical function and prevent repeated injury.</p><p><strong>Aim: </strong>To determine whether BFR is more effective than traditional rehabilitation in improving muscle strength, size, and stability after foot and ankle injury.</p><p><strong>Methods: </strong>A systematic review and meta-analysis were performed. Articles were retrieved from MEDLINE, EMBASE, and CENTRAL databases. Included studies compared the effectiveness of BFR rehabilitation to traditional foot and ankle rehabilitation exercises. Eligible patients were those with a history of foot or ankle injury. Muscle strength, size, and dynamic balance were assessed by comparing improvements in peak torque, cross-sectional area, and percent muscle activation. Methodological quality assessments were performed using the PEDro scale and Methodological Index for Non-Randomized Studies (MINORS).</p><p><strong>Results: </strong>Ten studies met the inclusion criteria. Five studies were of good to excellent quality according to the PEDro scale, and 5 studies were of moderate quality as per the MINORS criteria. Two studies compared the effect of BFR and non-BFR rehabilitation on muscle strength; the overall mean difference between the BRF and non-BFR groups was 0.09 [95%CI: (0.05, 0.12), <i>P</i> < 0.0001]. Two studies analyzed muscle activation following BFR and non-BFR rehabilitation; the overall mean difference between the BRF and non-BFR groups was 0.09 [95%CI: (0.05, 0.12), <i>P</i> < 0.0001]. Data on dynamic balance was synthesized from two studies; the mean difference between the BFR and control groups was 1.23 [95%CI: (-1.55, 4.01); <i>P</i> = 0.39].</p><p><strong>Conclusion: </strong>BFR rehabilitation is more effective than non-BFR rehabilitation at improving muscle strength and activation following foot and ankle injury. Additional studies are needed to develop a standardized BFR training protocol.</p>","PeriodicalId":47843,"journal":{"name":"World Journal of Orthopedics","volume":"16 6","pages":"106804"},"PeriodicalIF":2.3000,"publicationDate":"2025-06-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12179901/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Orthopedics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5312/wjo.v16.i6.106804","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Poor musculoskeletal recovery following foot and ankle injury can result in chronic instability and persistent muscle weakness. Preliminary evidence has shown that blood flow restriction (BFR) rehabilitation can increase muscle strength and stability, helping to restore physical function and prevent repeated injury.
Aim: To determine whether BFR is more effective than traditional rehabilitation in improving muscle strength, size, and stability after foot and ankle injury.
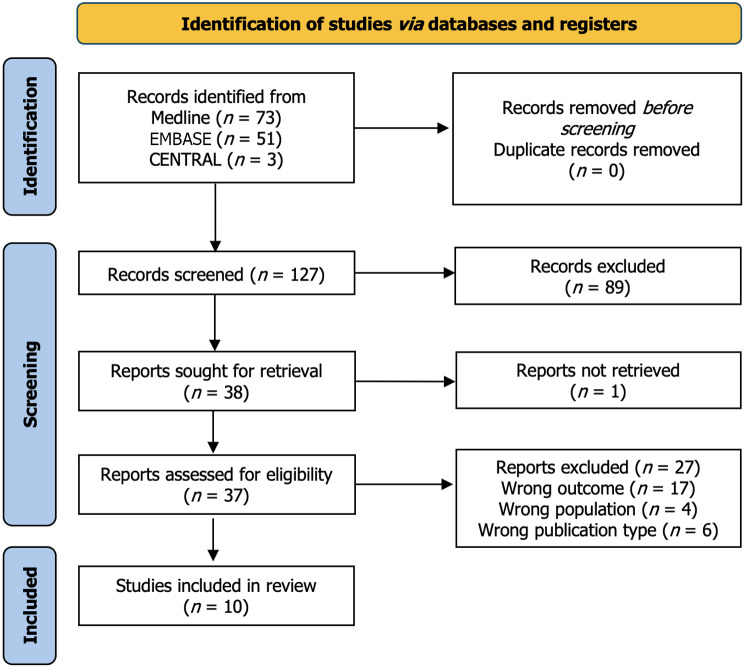
Methods: A systematic review and meta-analysis were performed. Articles were retrieved from MEDLINE, EMBASE, and CENTRAL databases. Included studies compared the effectiveness of BFR rehabilitation to traditional foot and ankle rehabilitation exercises. Eligible patients were those with a history of foot or ankle injury. Muscle strength, size, and dynamic balance were assessed by comparing improvements in peak torque, cross-sectional area, and percent muscle activation. Methodological quality assessments were performed using the PEDro scale and Methodological Index for Non-Randomized Studies (MINORS).
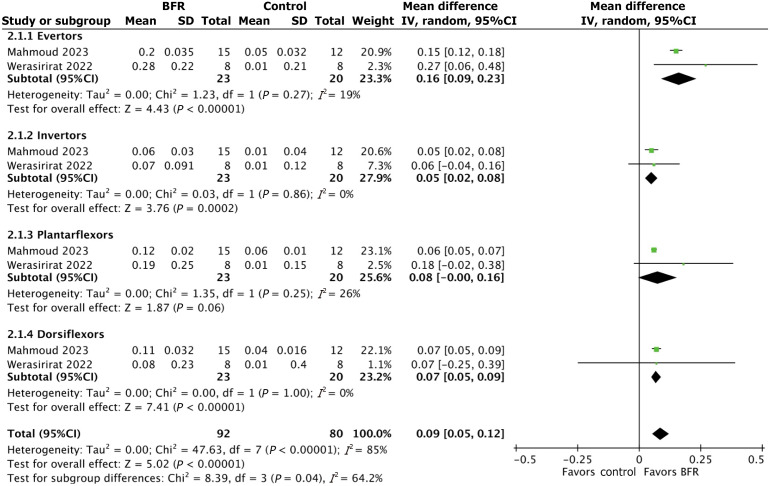
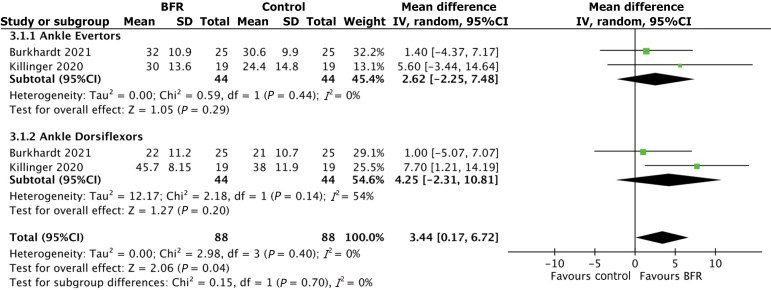
Results: Ten studies met the inclusion criteria. Five studies were of good to excellent quality according to the PEDro scale, and 5 studies were of moderate quality as per the MINORS criteria. Two studies compared the effect of BFR and non-BFR rehabilitation on muscle strength; the overall mean difference between the BRF and non-BFR groups was 0.09 [95%CI: (0.05, 0.12), P < 0.0001]. Two studies analyzed muscle activation following BFR and non-BFR rehabilitation; the overall mean difference between the BRF and non-BFR groups was 0.09 [95%CI: (0.05, 0.12), P < 0.0001]. Data on dynamic balance was synthesized from two studies; the mean difference between the BFR and control groups was 1.23 [95%CI: (-1.55, 4.01); P = 0.39].
Conclusion: BFR rehabilitation is more effective than non-BFR rehabilitation at improving muscle strength and activation following foot and ankle injury. Additional studies are needed to develop a standardized BFR training protocol.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


