{"title":"Advancing hemostasis: A meta-analysis of novel <i>vs</i> conventional endoscopic therapies for non variceal upper gastrointestinal bleeding.","authors":"Shivangini Duggal, Ishana Kalra, Keisha Kalra, Vicky Bhagat","doi":"10.4253/wjge.v17.i6.107142","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Non variceal upper gastrointestinal bleeding (NVUGIB) is a life-threatening condition requiring prompt and effective hemostasis. Various endoscopic interventions, including novel hemostatic powders (HP), over-the-scope clips (OTSC), and traditional approaches, have been employed to manage upper gastrointestinal bleeding (UGIB). Despite advancements, comparative efficacy and safety of these modalities remain uncertain.</p><p><strong>Aim: </strong>To evaluate the efficacy and safety of novel hemostatic interventions compared to conventional endoscopic techniques for managing UGIB.</p><p><strong>Methods: </strong>Cochrane, MEDLINE, PubMed and Scopus libraries were searched for randomized controlled trials (RCTs) published up to October 2024. Only RCTs comparing novel interventions, such as HP or OTSC, with conventional endoscopic treatments computed tomography (CT) were included. The primary outcome was the 30-day rebleeding rate. Secondary outcomes included initial hemostasis, short-term rebleeding rates, need for salvage therapy (surgical/angiographic), 30-day all-cause mortality, and bleeding-related mortality. We performed pairwise and network meta- analyses for all treatments.</p><p><strong>Results: </strong>Seventeen studies were included in this analysis. Regarding the 30-day rebleeding rate, OTSC and HP showed superior efficacy compared with CT [OTSC <i>vs</i> CT: Relative risk (RR): 0.47, 95% confidence interval (CI): 0.33-0.65; HP <i>vs</i> CT: RR: 0.73, 95%CI: 0.45-1.13], while OTSC and HP had comparable efficacy (RR: 0.56, 95%CI: 0.30-1.05). OTSC ranked the highest in the network ranking estimate for this outcome. For the secondary outcomes, OTSC demonstrated superior efficacy for the short-term rebleeding rate (OTSC <i>vs</i> CT: RR: 0.35, 95%CI: 0.14-0.74; HP <i>vs</i> CT: RR: 0.62, 95%CI: 0.28-1.35; OTSC <i>vs</i> HP: RR: 0.59, 95%CI: 0.17-1.67). Regarding the initial hemostasis rate, OTSC was slightly more effective than CT (OTSC <i>vs</i> CT: RR: 1.20, 95%CI: 1.06-1.57) and comparable to HP (OTSC <i>vs</i> HP: RR: 1.08, 95%CI: 0.89-1.40). There were no significant differences among treatments for all-cause mortality, bleeding-related mortality, or the necessity of surgical or angiographic salvage therapy. OTSC consistently ranked highest across most outcomes in the network ranking estimate.</p><p><strong>Conclusion: </strong>This meta-analysis highlights OTSC as the most effective intervention for reducing 30-day and short-term rebleeding rates in NVUGIB, surpassing both CT and HP, supporting OTSC as a preferred first-line treatment for NVUGIB, while HP and CT remain viable alternatives. Further studies are needed to explore long-term outcomes and cost-effectiveness.</p>","PeriodicalId":23953,"journal":{"name":"World Journal of Gastrointestinal Endoscopy","volume":"17 6","pages":"107142"},"PeriodicalIF":1.8000,"publicationDate":"2025-06-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12179957/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4253/wjge.v17.i6.107142","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Non variceal upper gastrointestinal bleeding (NVUGIB) is a life-threatening condition requiring prompt and effective hemostasis. Various endoscopic interventions, including novel hemostatic powders (HP), over-the-scope clips (OTSC), and traditional approaches, have been employed to manage upper gastrointestinal bleeding (UGIB). Despite advancements, comparative efficacy and safety of these modalities remain uncertain.
Aim: To evaluate the efficacy and safety of novel hemostatic interventions compared to conventional endoscopic techniques for managing UGIB.
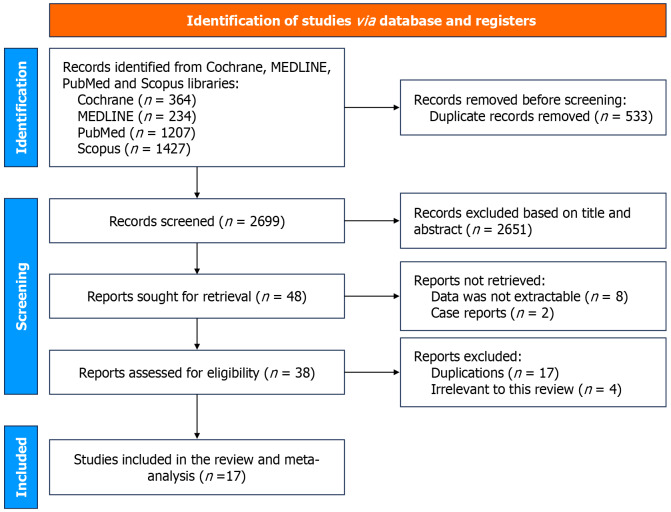
Methods: Cochrane, MEDLINE, PubMed and Scopus libraries were searched for randomized controlled trials (RCTs) published up to October 2024. Only RCTs comparing novel interventions, such as HP or OTSC, with conventional endoscopic treatments computed tomography (CT) were included. The primary outcome was the 30-day rebleeding rate. Secondary outcomes included initial hemostasis, short-term rebleeding rates, need for salvage therapy (surgical/angiographic), 30-day all-cause mortality, and bleeding-related mortality. We performed pairwise and network meta- analyses for all treatments.
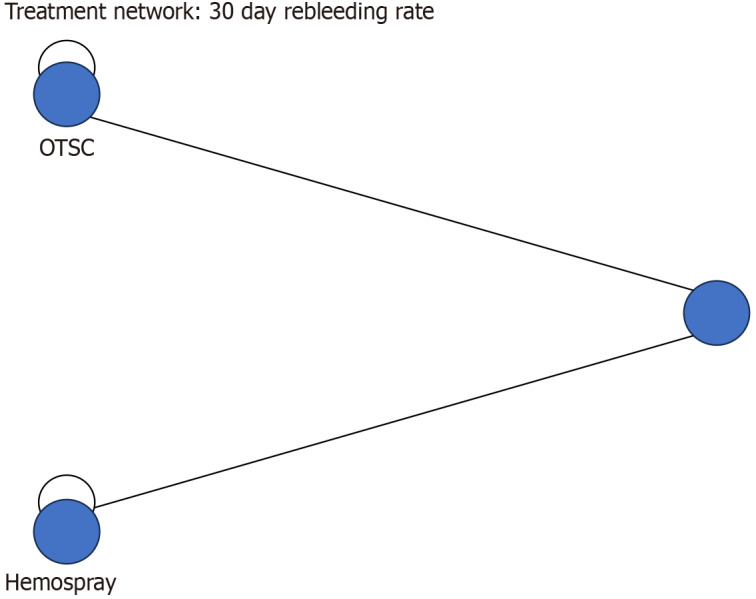
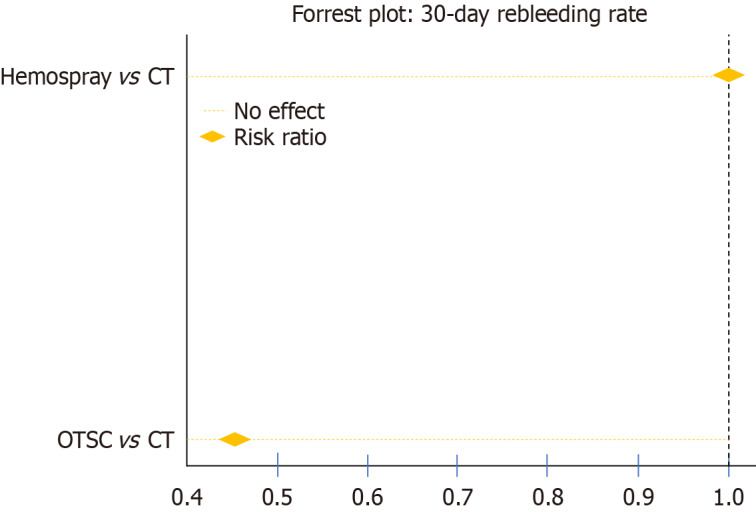
Results: Seventeen studies were included in this analysis. Regarding the 30-day rebleeding rate, OTSC and HP showed superior efficacy compared with CT [OTSC vs CT: Relative risk (RR): 0.47, 95% confidence interval (CI): 0.33-0.65; HP vs CT: RR: 0.73, 95%CI: 0.45-1.13], while OTSC and HP had comparable efficacy (RR: 0.56, 95%CI: 0.30-1.05). OTSC ranked the highest in the network ranking estimate for this outcome. For the secondary outcomes, OTSC demonstrated superior efficacy for the short-term rebleeding rate (OTSC vs CT: RR: 0.35, 95%CI: 0.14-0.74; HP vs CT: RR: 0.62, 95%CI: 0.28-1.35; OTSC vs HP: RR: 0.59, 95%CI: 0.17-1.67). Regarding the initial hemostasis rate, OTSC was slightly more effective than CT (OTSC vs CT: RR: 1.20, 95%CI: 1.06-1.57) and comparable to HP (OTSC vs HP: RR: 1.08, 95%CI: 0.89-1.40). There were no significant differences among treatments for all-cause mortality, bleeding-related mortality, or the necessity of surgical or angiographic salvage therapy. OTSC consistently ranked highest across most outcomes in the network ranking estimate.
Conclusion: This meta-analysis highlights OTSC as the most effective intervention for reducing 30-day and short-term rebleeding rates in NVUGIB, surpassing both CT and HP, supporting OTSC as a preferred first-line treatment for NVUGIB, while HP and CT remain viable alternatives. Further studies are needed to explore long-term outcomes and cost-effectiveness.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


