Intratympanic steroid injection adjunct to myringotomy with ventilation tube insertion for otitis media with effusion in children with cleft palate - a matched pair randomized controlled trial.
{"title":"Intratympanic steroid injection adjunct to myringotomy with ventilation tube insertion for otitis media with effusion in children with cleft palate - a matched pair randomized controlled trial.","authors":"Patorn Piromchai, Jutarat Anutragulchai, Kwanchanok Yimtae, Somchai Srirompotong, Panida Thanawirattananit","doi":"10.1177/20503121251348026","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>To evaluate the efficacy of adjunctive intratympanic dexamethasone therapy in improving outcomes of myringotomy with ventilation tube insertion for bilateral otitis media with effusion in children with cleft palate.</p><p><strong>Methods: </strong>Children with cleft palate aged 2-12 years were recruited. Dexamethasone or placebo was administered intratympanically based on randomized allocation, with contralateral ear receiving the alternate treatment.</p><p><strong>Results: </strong>Twenty-three children with cleft palate (mean age: 33.04 ± 27.80 months) were enrolled. Baseline demographics were comparable between groups (<i>p</i> > 0.05). Both dexamethasone and placebo groups demonstrated significant hearing level improvements at 1-month follow-up (<i>p</i> < 0.001). Patients with otitis media with effusion duration ⩽ 3 months exhibited superior outcomes in the dexamethasone group (mean difference: -3.18 dB HL, 95% CI: -4.88 to -1.49, <i>p</i> = 0.002). Patients with cleft palate without other anomalies demonstrated a significant improvement in the dexamethasone group (mean difference: -3.24 dB HL, 95% CI: -5.04 to -1.43, <i>p</i> = 0.002). No significant differences in adverse events were observed between groups (<i>p</i> > 0.05).</p><p><strong>Conclusions: </strong>Early intratympanic dexamethasone injection adjunct to myringotomy with ventilation tube insertion is recommended for otitis media with effusion in children with cleft palate.</p>","PeriodicalId":21398,"journal":{"name":"SAGE Open Medicine","volume":"13 ","pages":"20503121251348026"},"PeriodicalIF":2.1000,"publicationDate":"2025-06-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12179480/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"SAGE Open Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20503121251348026","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: To evaluate the efficacy of adjunctive intratympanic dexamethasone therapy in improving outcomes of myringotomy with ventilation tube insertion for bilateral otitis media with effusion in children with cleft palate.
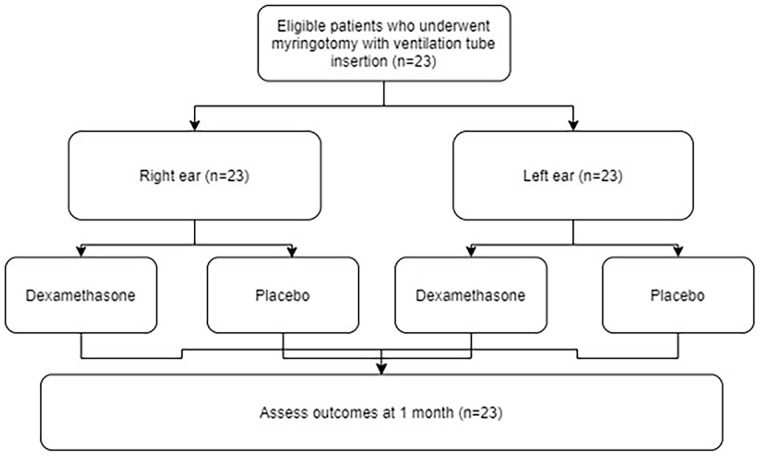
Methods: Children with cleft palate aged 2-12 years were recruited. Dexamethasone or placebo was administered intratympanically based on randomized allocation, with contralateral ear receiving the alternate treatment.
Results: Twenty-three children with cleft palate (mean age: 33.04 ± 27.80 months) were enrolled. Baseline demographics were comparable between groups (p > 0.05). Both dexamethasone and placebo groups demonstrated significant hearing level improvements at 1-month follow-up (p < 0.001). Patients with otitis media with effusion duration ⩽ 3 months exhibited superior outcomes in the dexamethasone group (mean difference: -3.18 dB HL, 95% CI: -4.88 to -1.49, p = 0.002). Patients with cleft palate without other anomalies demonstrated a significant improvement in the dexamethasone group (mean difference: -3.24 dB HL, 95% CI: -5.04 to -1.43, p = 0.002). No significant differences in adverse events were observed between groups (p > 0.05).
Conclusions: Early intratympanic dexamethasone injection adjunct to myringotomy with ventilation tube insertion is recommended for otitis media with effusion in children with cleft palate.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


